

Partial and generalized lipodystrophy: comparison of baseline characteristics and response to metreleptin
- PMID: 25734254
- PMCID: PMC4422900
- DOI: 10.1210/jc.2014-4491
Partial and generalized lipodystrophy: comparison of baseline characteristics and response to metreleptin
Abstract
Context: Lipodystrophies are extreme forms of metabolic syndrome. Metreleptin was approved in the United States for generalized lipodystrophy (GLD) but not partial lipodystrophy (PLD).
Objective: The objective of the study was to test metreleptin's efficacy in PLD vs GLD and find predictors for treatment response.
Design: This was a prospective, single-arm, open-label study since 2000 with continuous enrollment. Current analysis included metreleptin treatment for 6 months or longer as of January 2014.
Setting: The study was conducted at the National Institutes of Health (Bethesda, Maryland).
Participants: Patients clinically diagnosed with lipodystrophy, leptin less than 8 ng/mL (males) or less than 12 (females), age older than 6 months, and one or more metabolic abnormalities (diabetes, insulin resistance, or hypertriglyceridemia) participated in the study.
Intervention: The interventions included sc metreleptin injections (0.06-0.24 mg/kg · d).
Main outcomes and measures: Changes in glycated hemoglobin A1c (HbA1c) and triglycerides after 6 and 12 months of metreleptin were measured.
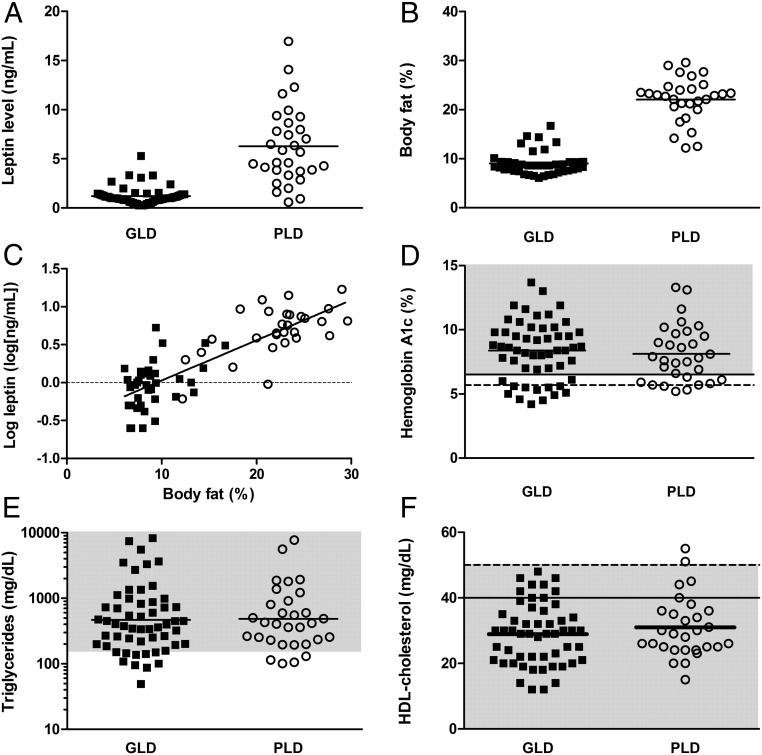
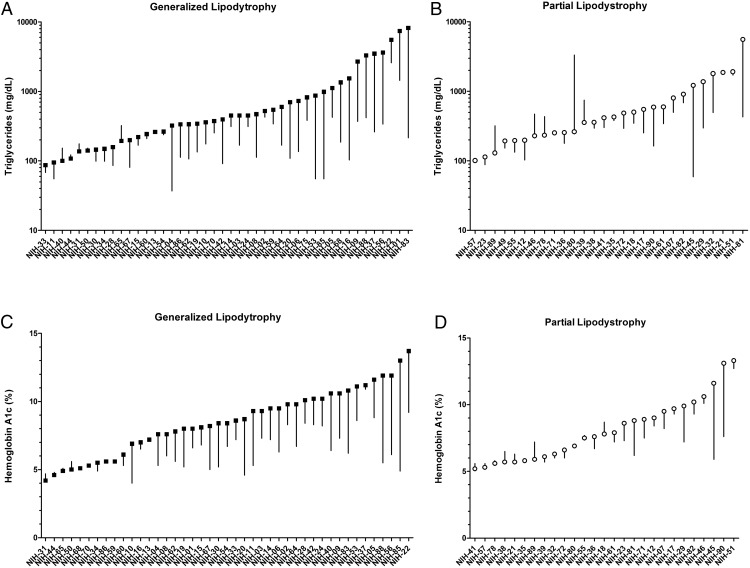
Results: Baseline metabolic parameters were similar in 55 GLD [HbA1c 8.4% ± 2.3%; triglycerides, geometric mean (25th, 75th percentile), 467 mg/dL (200, 847)] and 31 PLD patients [HbA1c 8.1% ± 2.2%, triglycerides 483 mg/dL (232, 856)] despite different body fat and endogenous leptin. At 12 months, metreleptin decreased HbA1c (to 6.4% ± 1.5%, GLD, P < .001; 7.3% ± 1.6%, PLD, P = .004) and triglycerides [to 180 mg/dL (106, 312), GLD, P < .001; 326 mg/dL (175, 478), PLD, P = .02]. HbA1c and triglyceride changes over time significantly differed between GLD and PLD. In subgroup analyses, metreleptin improved HbA1c and triglycerides in all GLD subgroups except those with baseline triglycerides less than 300 mg/dL and all PLD subgroups except baseline triglycerides less than 500 mg/dL, HbA1c less than 8%, or endogenous leptin greater than 4 ng/mL.
Conclusions: In addition to its proven efficacy in GLD, metreleptin is effective in selected PLD patients with severe metabolic derangements or low leptin.
Trial registration: ClinicalTrials.gov NCT00025883.
Figures
References
-
- Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120:1640–1645. - PubMed
-
- Haque WA, Shimomura I, Matsuzawa Y, Garg A. Serum adiponectin and leptin levels in patients with lipodystrophies. J Clin Endocrinol Metab. 2002;87:2395. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
