

Global epidemiology of pediatric severe sepsis: the sepsis prevalence, outcomes, and therapies study
- PMID: 25734408
- PMCID: PMC4451622
- DOI: 10.1164/rccm.201412-2323OC
Global epidemiology of pediatric severe sepsis: the sepsis prevalence, outcomes, and therapies study
Erratum in
-
Erratum: Global Epidemiology of Pediatric Severe Sepsis: The Sepsis Prevalence, Outcomes, and Therapies Study.Am J Respir Crit Care Med. 2016 Jan 15;193(2):223-4. doi: 10.1164/rccm.1932erratum. Am J Respir Crit Care Med. 2016. PMID: 26771421 Free PMC article. No abstract available.
Abstract
Rationale: Limited data exist about the international burden of severe sepsis in critically ill children.
Objectives: To characterize the global prevalence, therapies, and outcomes of severe sepsis in pediatric intensive care units to better inform interventional trials.
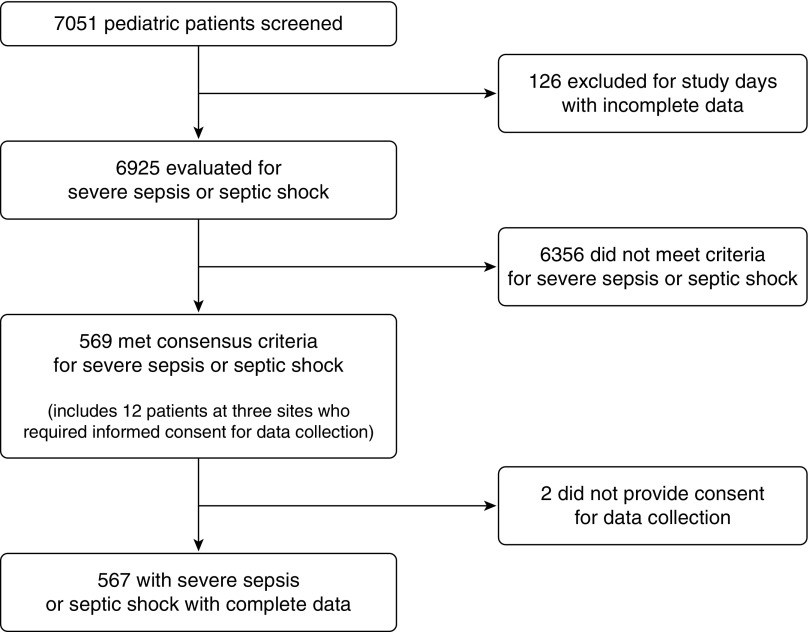
Methods: A point prevalence study was conducted on 5 days throughout 2013-2014 at 128 sites in 26 countries. Patients younger than 18 years of age with severe sepsis as defined by consensus criteria were included. Outcomes were severe sepsis point prevalence, therapies used, new or progressive multiorgan dysfunction, ventilator- and vasoactive-free days at Day 28, functional status, and mortality.
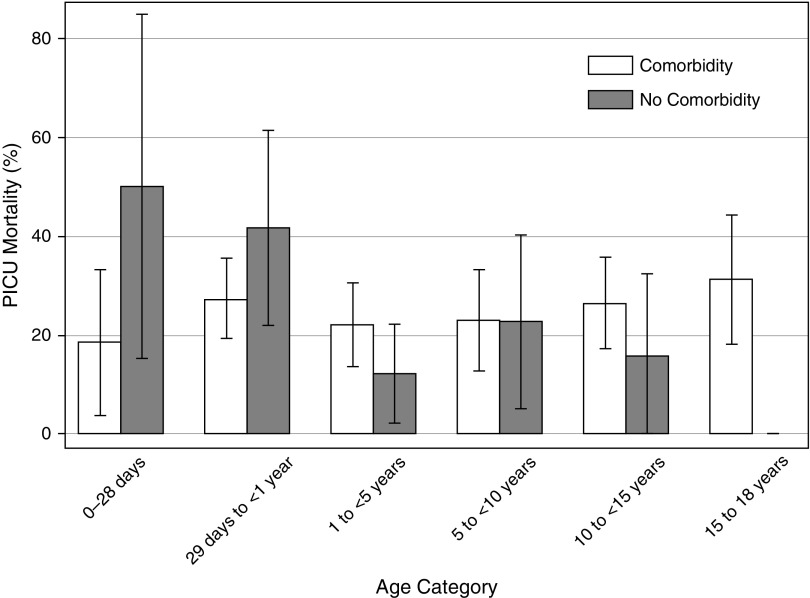
Measurements and main results: Of 6,925 patients screened, 569 had severe sepsis (prevalence, 8.2%; 95% confidence interval, 7.6-8.9%). The patients' median age was 3.0 (interquartile range [IQR], 0.7-11.0) years. The most frequent sites of infection were respiratory (40%) and bloodstream (19%). Common therapies included mechanical ventilation (74% of patients), vasoactive infusions (55%), and corticosteroids (45%). Hospital mortality was 25% and did not differ by age or between developed and resource-limited countries. Median ventilator-free days were 16 (IQR, 0-25), and vasoactive-free days were 23 (IQR, 12-28). Sixty-seven percent of patients had multiorgan dysfunction at sepsis recognition, with 30% subsequently developing new or progressive multiorgan dysfunction. Among survivors, 17% developed at least moderate disability. Sample sizes needed to detect a 5-10% absolute risk reduction in outcomes within interventional trials are estimated between 165 and 1,471 [corrected] patients per group.
Conclusions: Pediatric severe sepsis remains a burdensome public health problem, with prevalence, morbidity, and mortality rates similar to those reported in critically ill adult populations. International clinical trials targeting children with severe sepsis are warranted.
Keywords: multiple organ failure; pediatrics; sepsis.
Figures
Comment in
-
Understanding the global burden of pediatric sepsis.Am J Respir Crit Care Med. 2015 May 15;191(10):1096-8. doi: 10.1164/rccm.201503-0594ED. Am J Respir Crit Care Med. 2015. PMID: 25978567 No abstract available.
References
-
- Hartman ME, Linde-Zwirble WT, Angus DC, Watson RS. Trends in the epidemiology of pediatric severe sepsis. Pediatr Crit Care Med. 2013;14:686–693. - PubMed
-
- Jaramillo-Bustamante JC, Marín-Agudelo A, Fernández-Laverde M, Bareño-Silva J. Epidemiology of sepsis in pediatric intensive care units: first Colombian multicenter study. Pediatr Crit Care Med. 2012;13:501–508. - PubMed
-
- Kutko MC, Calarco MP, Flaherty MB, Helmrich RF, Ushay HM, Pon S, Greenwald BM. Mortality rates in pediatric septic shock with and without multiple organ system failure. Pediatr Crit Care Med. 2003;4:333–337. - PubMed
-
- Watson RS, Carcillo JA, Linde-Zwirble WT, Clermont G, Lidicker J, Angus DC. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med. 2003;167:695–701. - PubMed
-
- Weiss SL, Parker B, Bullock ME, Swartz S, Price C, Wainwright MS, Goodman DM. Defining pediatric sepsis by different criteria: discrepancies in populations and implications for clinical practice. Pediatr Crit Care Med. 2012;13:e219–e226. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
