

A systematic review and meta-analysis of premature mortality in bipolar affective disorder
- PMID: 25735195
- PMCID: PMC4939858
- DOI: 10.1111/acps.12408
A systematic review and meta-analysis of premature mortality in bipolar affective disorder
Abstract
Objective: To review and complete meta-analysis of studies estimating standardised mortality ratios (SMRs) in bipolar affective disorder (BPAD) for all-cause and cause-specific mortalities.
Method: Cause-specific mortality was grouped into natural and unnatural causes. These subgroups were further divided into circulatory, respiratory, neoplastic and infectious causes, and suicide and other violent deaths. Summary SMRs were calculated using random-effects meta-analysis. Heterogeneity was examined via subgroup analysis and meta-regression.
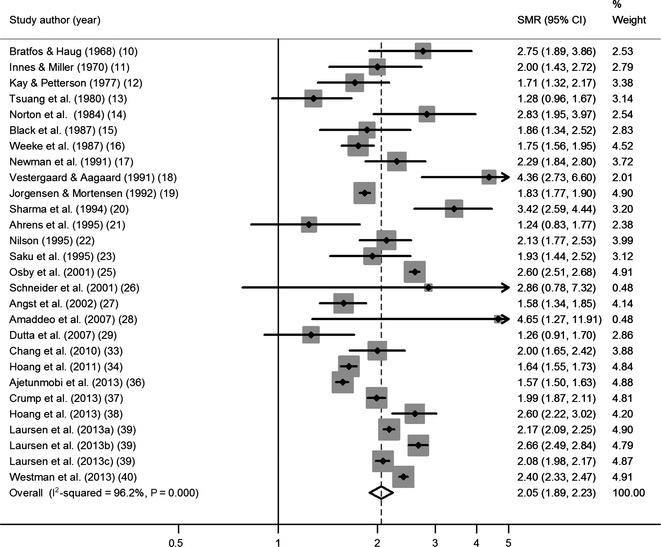
Results: Systematic searching found 31 studies meeting inclusion criteria. Summary SMR for all-cause mortality = 2.05 (95% CI 1.89-2.23), but heterogeneity was high (I(2) = 96.2%). This heterogeneity could not be accounted for by date of publication, cohort size, mid-decade of data collection, population type or geographical region. Unnatural death summary SMR = 7.42 (95% CI 6.43-8.55) and natural death = 1.64 (95% CI 1.47-1.83). Specifically, suicide SMR = 14.44 (95% CI 12.43-16.78), other violent death SMR = 3.68 (95% CI 2.77-4.90), deaths from circulatory disease = 1.73 (95% CI 1.54-1.94), respiratory disease = 2.92 (95% CI 2.00-4.23), infection = 2.25 (95% CI 1.70-3.00) and neoplasm = 1.14 (95% CI 1.10-1.21).
Conclusion: Despite considerable heterogeneity, all summary SMR estimates and a large majority of individual studies showed elevated mortality in BPAD compared to the general population. This was true for all causes of mortality studied.
Keywords: bipolar disorder; life expectancy; mortality.
© 2015 The Authors. Acta Psychiatrica Scandinavica Published by John Wiley & Sons Ltd.
Figures

Comment in
-
Critique of a systematic review and meta-analysis of premature mortality in bipolar affective disorder.Acta Psychiatr Scand. 2015 Oct;132(4):315. doi: 10.1111/acps.12432. Epub 2015 May 5. Acta Psychiatr Scand. 2015. PMID: 25943589 No abstract available.
-
Reply: To PMID 25735195.Acta Psychiatr Scand. 2015 Oct;132(4):315-6. doi: 10.1111/acps.12438. Epub 2015 May 5. Acta Psychiatr Scand. 2015. PMID: 25943709 No abstract available.
References
-
- Roshanaei‐Moghaddam B, Katon W. Premature mortality from general medical illnesses among persons with bipolar disorder: a review. Psychiatr Serv 2009;60:147–156. - PubMed
-
- Harris EC, Barraclough B. Excess mortality of mental disorder. Br J Psychiatry 1998;173:11–53. - PubMed
-
- McIntyre RS, Soczynska JK, Beyer JL et al. Medical comorbidity in bipolar disorder: reprioritizing unmet needs. Curr Opin Psychiatry 2007;20:406–416. - PubMed
-
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. Ann Intern Med 2009;151:264–269. - PubMed
-
- Stroup DF, Berlin JA, Morton SC et al. Meta‐analysis of observational studies in epidemiology: a proposal for reporting. JAMA 2000;283:2008–2012. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
