

Alternative calculations of individual patient time in therapeutic range while taking warfarin: results from the ROCKET AF trial
- PMID: 25736441
- PMCID: PMC4392426
- DOI: 10.1161/JAHA.114.001349
Alternative calculations of individual patient time in therapeutic range while taking warfarin: results from the ROCKET AF trial
Abstract
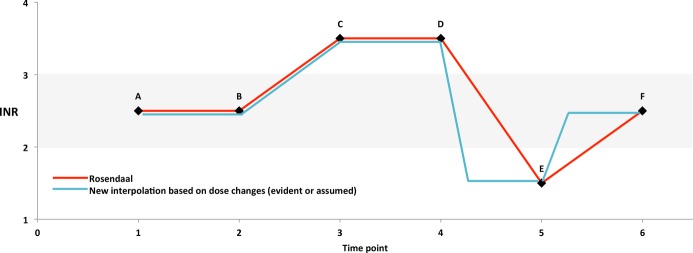
Background: In the ROCKET AF (Rivaroxaban-Once-daily, oral, direct Factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation) trial, marked regional differences in control of warfarin anticoagulation, measured as the average individual patient time in the therapeutic range (iTTR) of the international normalized ratio (INR), were associated with longer inter-INR test intervals. The standard Rosendaal approach can produce biased low estimates of TTR after an appropriate dose change if the follow-up INR test interval is prolonged. We explored the effect of alternative calculations of TTR that more immediately account for dose changes on regional differences in mean iTTR in the ROCKET AF trial.
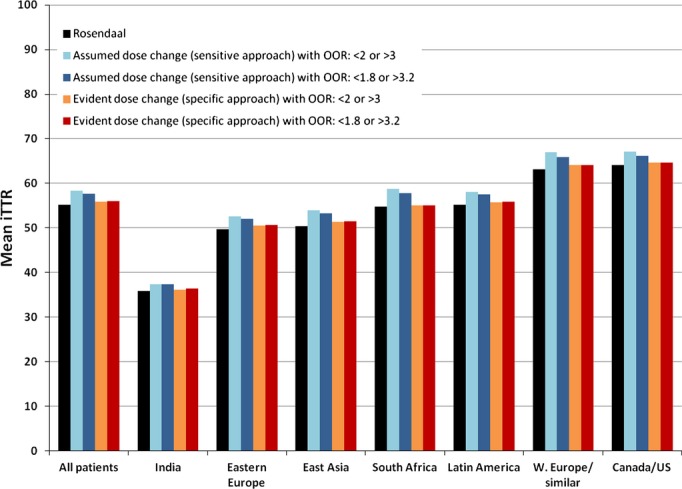
Methods and results: We used an INR imputation method that accounts for dose change. We compared group mean iTTR values between our dose change-based method with the standard Rosendaal method and determined that the differences between approaches depended on the balance of dose changes that produced in-range INRs ("corrections") versus INRs that were out of range in the opposite direction ("overshoots"). In ROCKET AF, the overall mean iTTR of 55.2% (Rosendaal) increased up to 3.1% by using the dose change-based approach, depending on assumptions. However, large inter-regional differences in anticoagulation control persisted.
Conclusions: TTR, the standard measure of control of warfarin anticoagulation, depends on imputing daily INR values for the vast majority of follow-up days. Our TTR calculation method may better reflect the impact of warfarin dose changes than the Rosendaal approach. In the ROCKET AF trial, this dose change-based approach led to a modest increase in overall mean iTTR but did not materially affect the large inter-regional differences previously reported.
Clinical trial registration: URL: ClinicalTrials.gov. Unique identifier: NCT00403767.
Keywords: anticoagulants; arrhythmia; embolism; prevention; risk factors.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Rosendaal FR, Cannegieter SC, van der Meer FJ, Briet E. A method to determine the optimal intensity of oral anticoagulant therapy. Thromb Haemost. 1993; 69:236-239. - PubMed
-
- Rose AJ, Hylek EM, Ozonoff A, Ash AS, Reisman JI, Berlowitz DR. Risk‐adjusted percent time in therapeutic range as a quality indicator for outpatient oral anticoagulation: results of the Veterans Affairs Study to Improve Anticoagulation (VARIA). Circ Cardiovasc Qual Outcomes. 2011; 4:22-29. - PubMed
-
- Dlott JS, George RA, Huang X, Odeh M, Kaufman HW, Ansell J, Hylek EM. National assessment of warfarin anticoagulation therapy for stroke prevention in atrial fibrillation. Circulation. 2014; 129:1407-1414. - PubMed
-
- Wieloch M, Sjalander A, Frykman V, Rosenqvist M, Eriksson N, Svensson PJ. Anticoagulation control in Sweden: reports of time in therapeutic range, major bleeding, and thrombo‐embolic complications from the national quality registry AuriculA. Eur Heart J. 2011; 32:2282-2289. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
