

The HEART Pathway randomized trial: identifying emergency department patients with acute chest pain for early discharge
- PMID: 25737484
- PMCID: PMC4413911
- DOI: 10.1161/CIRCOUTCOMES.114.001384
The HEART Pathway randomized trial: identifying emergency department patients with acute chest pain for early discharge
Abstract
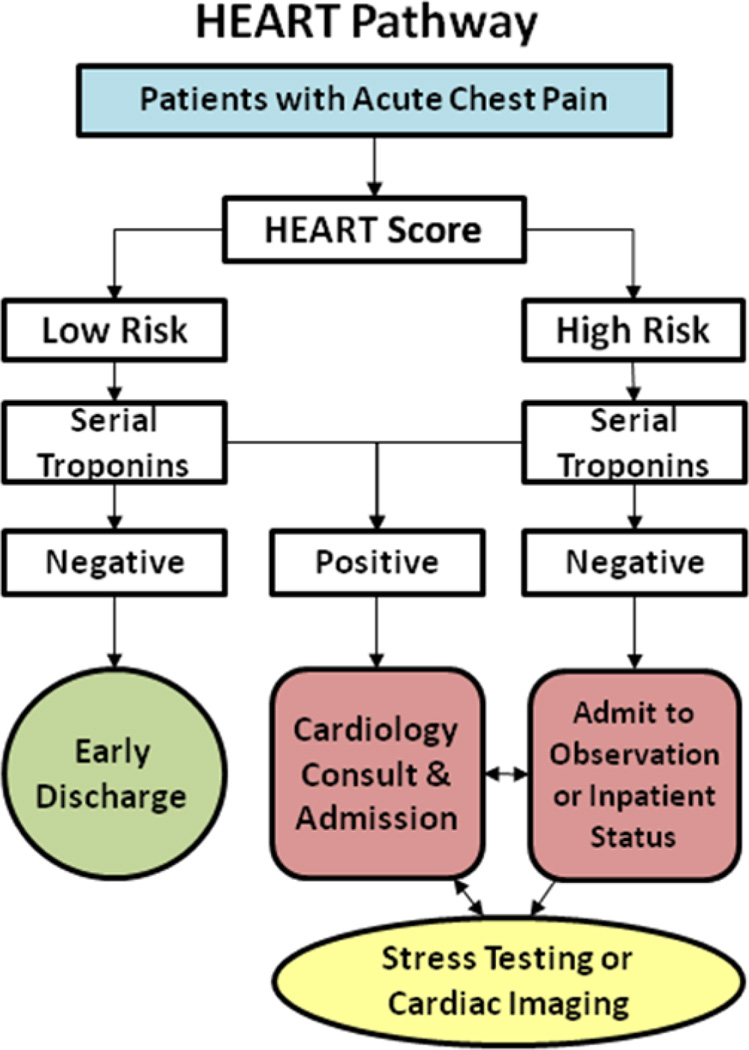
Background: The HEART Pathway is a decision aid designed to identify emergency department patients with acute chest pain for early discharge. No randomized trials have compared the HEART Pathway with usual care.
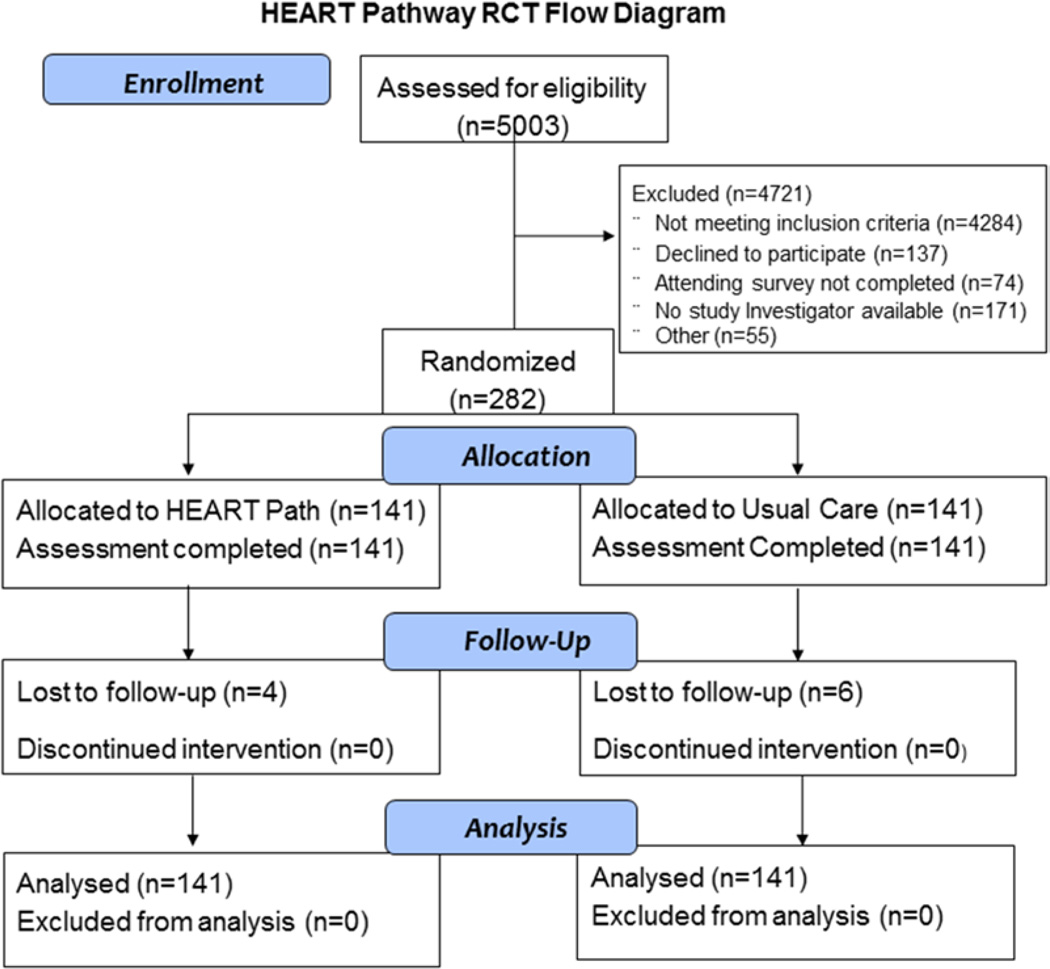
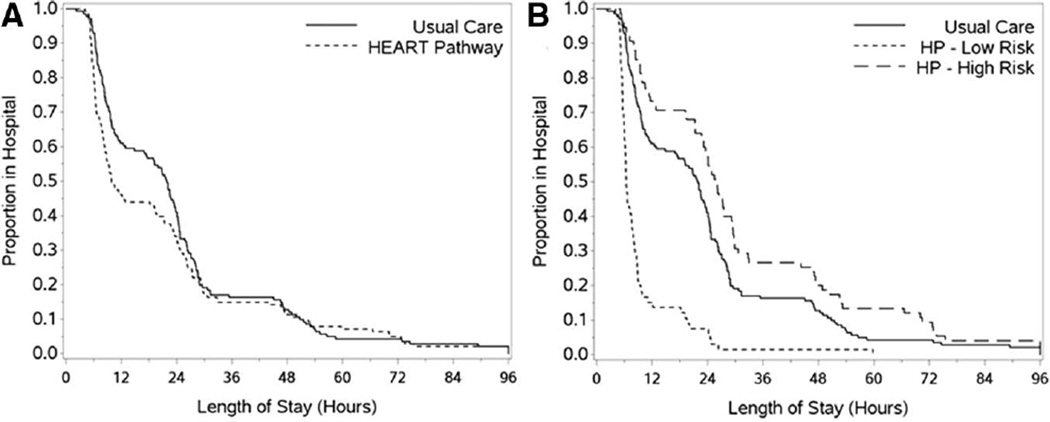
Methods and results: Adult emergency department patients with symptoms related to acute coronary syndrome without ST-elevation on ECG (n=282) were randomized to the HEART Pathway or usual care. In the HEART Pathway arm, emergency department providers used the HEART score, a validated decision aid, and troponin measures at 0 and 3 hours to identify patients for early discharge. Usual care was based on American College of Cardiology/American Heart Association guidelines. The primary outcome, objective cardiac testing (stress testing or angiography), and secondary outcomes, index length of stay, early discharge, and major adverse cardiac events (death, myocardial infarction, or coronary revascularization), were assessed at 30 days by phone interview and record review. Participants had a mean age of 53 years, 16% had previous myocardial infarction, and 6% (95% confidence interval, 3.6%-9.5%) had major adverse cardiac events within 30 days of randomization. Compared with usual care, use of the HEART Pathway decreased objective cardiac testing at 30 days by 12.1% (68.8% versus 56.7%; P=0.048) and length of stay by 12 hours (9.9 versus 21.9 hours; P=0.013) and increased early discharges by 21.3% (39.7% versus 18.4%; P<0.001). No patients identified for early discharge had major adverse cardiac events within 30 days.
Conclusions: The HEART Pathway reduces objective cardiac testing during 30 days, shortens length of stay, and increases early discharges. These important efficiency gains occurred without any patients identified for early discharge suffering MACE at 30 days.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique Identifier: NCT01665521.
Keywords: acute coronary syndrome; chest pain; clinical trial; decision support techniques.
© 2015 American Heart Association, Inc.
Figures
Comment in
-
Finding the holy grail is not a short-term project.Circ Cardiovasc Qual Outcomes. 2015 Mar;8(2):135-7. doi: 10.1161/CIRCOUTCOMES.115.001611. Epub 2015 Mar 3. Circ Cardiovasc Qual Outcomes. 2015. PMID: 25737489 No abstract available.
References
-
- Owens PL, Barrett ML, Gibson TB, Andrews RM, Weinick RM, Mutter RL. Emergency department care in the United States: a profile of national data sources. Ann Emerg Med. 2010;56:150–165. - PubMed
-
- Litt HI, Gatsonis C, Snyder B, Singh H, Miller CD, Entrikin DW, Leaming JM, Gavin LJ, Pacella CB, Hollander JE. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med. 2012;366:1393–1403. - PubMed
-
- Heller GV, Stowers SA, Hendel RC, Herman SD, Daher E, Ahlberg AW, Baron JM, Mendes de Leon CF, Rizzo JA, Wackers FJ. Clinical value of acute rest technetium-99m tetrofosmin tomographic myocardial perfusion imaging in patients with acute chest pain and nondiagnostic electrocardiograms. J Am Coll Cardiol. 1998;31:1011–1017. - PubMed
-
- Roberts R, Kleiman NS. Earlier diagnosis and treatment of acute myocardial infarction necessitates the need for a ‘new diagnostic mind-set’. Circulation. 1994;89:872–881. - PubMed
-
- Hoffmann U, Nagurney JT, Moselewski F, Pena A, Ferencik M, Chae CU, Cury RC, Butler J, Abbara S, Brown DF, Manini A, Nichols JH, Achenbach S, Brady TJ. Coronary multidetector computed tomography in the assessment of patients with acute chest pain. Circulation. 2006;114:2251–2260. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
