

Long-Term Behavioral Outcomes after a Randomized, Clinical Trial of Counselor-Assisted Problem Solving for Adolescents with Complicated Mild-to-Severe Traumatic Brain Injury
- PMID: 25738891
- PMCID: PMC4492777
- DOI: 10.1089/neu.2014.3684
Long-Term Behavioral Outcomes after a Randomized, Clinical Trial of Counselor-Assisted Problem Solving for Adolescents with Complicated Mild-to-Severe Traumatic Brain Injury
Abstract
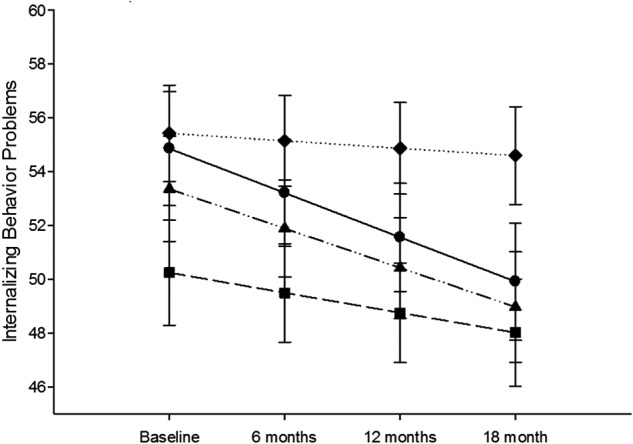
Family problem-solving therapy (FPST) has been shown to reduce behavior problems after pediatric traumatic brain injury (TBI). It is unclear whether treatment gains are maintained. We sought to evaluate the maintenance of improvements in behavior problems after a Web-based counselor-assisted FPST (CAPS) intervention compared to an Internet resource comparison (IRC) intervention provided to adolescents within the initial year post-TBI. We hypothesized that family socioeconomic status, child educational status, and baseline levels of symptoms would moderate the efficacy of the treatment over time. Participants included 132 adolescents ages 12-17 years who sustained a complicated mild-to-severe TBI 1-6 months before study enrollment. Primary outcomes were the Child Behavior Checklist Internalizing and Externalizing Totals. Mixed-models analyses, using random intercepts and slopes, were conducted to examine group differences over time. There was a significant group×time×grade interaction (F(1,304)=4.42; p=0.03) for internalizing problems, with high school-age participants in CAPS reporting significantly lower symptoms at 18 months postbaseline than those in the IRC. Post-hoc analyses to elucidate the nature of effects on internalizing problems revealed significant group×time×grade interactions for the anxious/depressed (p=0.03) and somatic complaints subscales (p=0.04). Results also indicated significant improvement over time for CAPS participants who reported elevated externalizing behavior problems at baseline (F(1, 310)=7.17; p=0.008). Findings suggest that CAPS may lead to long-term improvements in behavior problems among older adolescents and those with pretreatment symptoms.
Trial registration: ClinicalTrials.gov NCT00409448.
Keywords: adolescent; behavior; brain injury; child; online; therapy.
Figures




References
-
- Max J.E., Robin D.A., Lindgren S.D., Sato Y., Smith W.L., Mattheis P.J., Stierwalt J.A., and Castillo C.S. (1997). Traumatic brain injury in children and adolescents: psychiatric disorders at two years. J. Am. Acad. Child Adolesc. Psychiatry 36, 1278–1285 - PubMed
-
- Max J.E., Arndt S., Castillo C.S., Bokura H., Robin D.A., Lindgren S.D., Smith W.L., Jr., Sato Y., and Mattheis P.J. (1998). Attention-deficit hyperactivity symptomatology after traumatic brain injury: a prospective study. J. Am. Acad. Child Adolesc. Psychiatry 37, 841–847 - PubMed
-
- Schwartz L., Taylor H.G., Drotar D., Yeates K.O., Wade S.L., and Stancin T. (2003). Long-term behavior problems following pediatric traumatic brain injury: prevalence, predictors, and correlates. J. Pediatr. Psychol. 28, 251–263 - PubMed
-
- Brown F.L., Whittingham K., Boyd R., and Sofronoff K. (2013). A systematic review of parenting interventions for traumatic brain injury: child and parent outcomes. J. Head Trauma Rehabil. 28, 349–360 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
