

The diagnostic accuracy of the natriuretic peptides in heart failure: systematic review and diagnostic meta-analysis in the acute care setting
- PMID: 25740799
- PMCID: PMC4353288
- DOI: 10.1136/bmj.h910
The diagnostic accuracy of the natriuretic peptides in heart failure: systematic review and diagnostic meta-analysis in the acute care setting
Abstract
Objectives: To determine and compare the diagnostic accuracy of serum natriuretic peptide levels (B type natriuretic peptide, N terminal probrain natriuretic peptide (NTproBNP), and mid-regional proatrial natriuretic peptide (MRproANP)) in people presenting with acute heart failure to acute care settings using thresholds recommended in the 2012 European Society of Cardiology guidelines for heart failure.
Design: Systematic review and diagnostic meta-analysis.
Data sources: Medline, Embase, Cochrane central register of controlled trials, Cochrane database of systematic reviews, database of abstracts of reviews of effects, NHS economic evaluation database, and Health Technology Assessment up to 28 January 2014, using combinations of subject headings and terms relating to heart failure and natriuretic peptides.
Eligibility criteria for selecting studies: Eligible studies evaluated one or more natriuretic peptides (B type natriuretic peptide, NTproBNP, or MRproANP) in the diagnosis of acute heart failure against an acceptable reference standard in consecutive or randomly selected adults in an acute care setting. Studies were excluded if they did not present sufficient data to extract or calculate true positives, false positives, false negatives, and true negatives, or report age independent natriuretic peptide thresholds. Studies not available in English were also excluded.
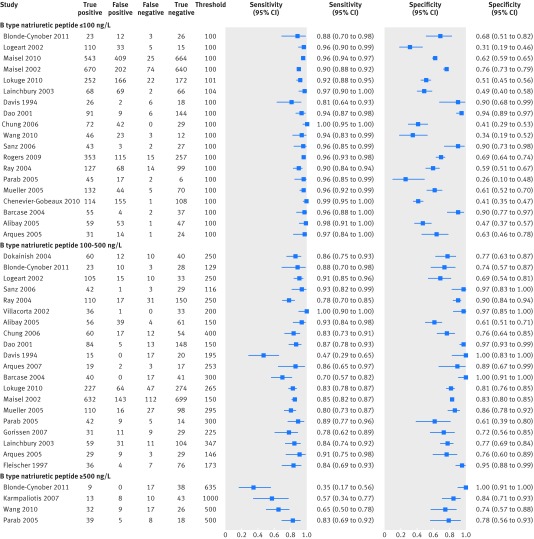
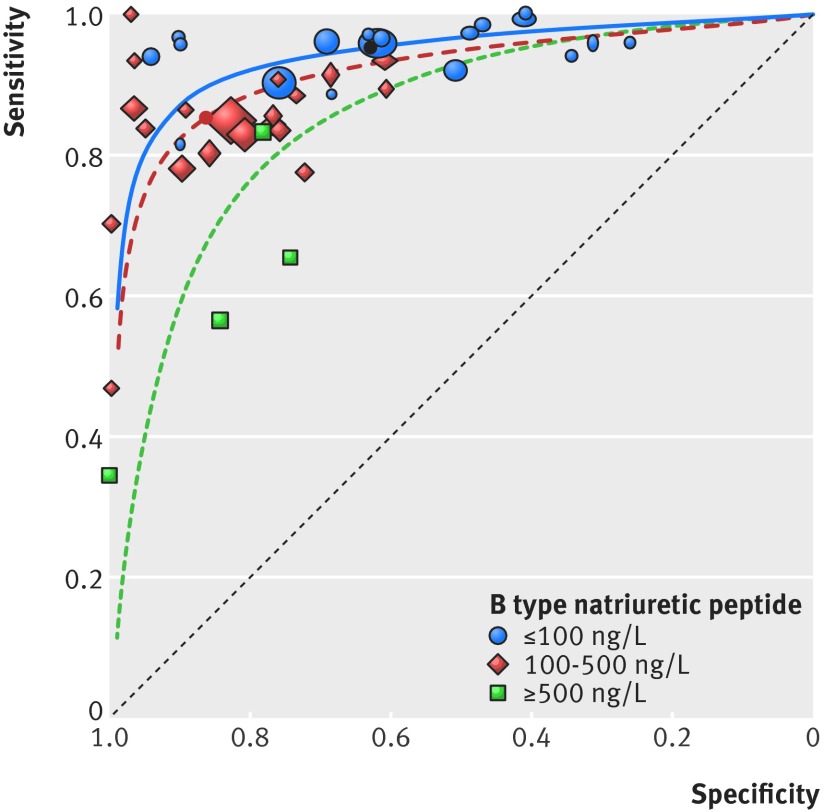
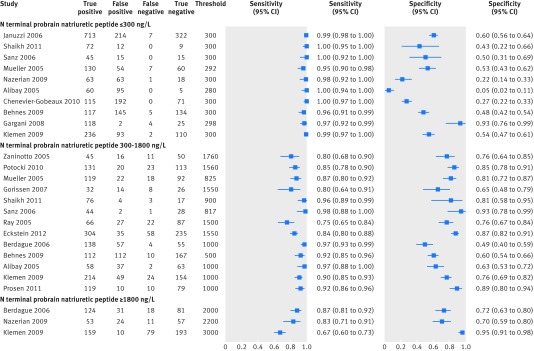
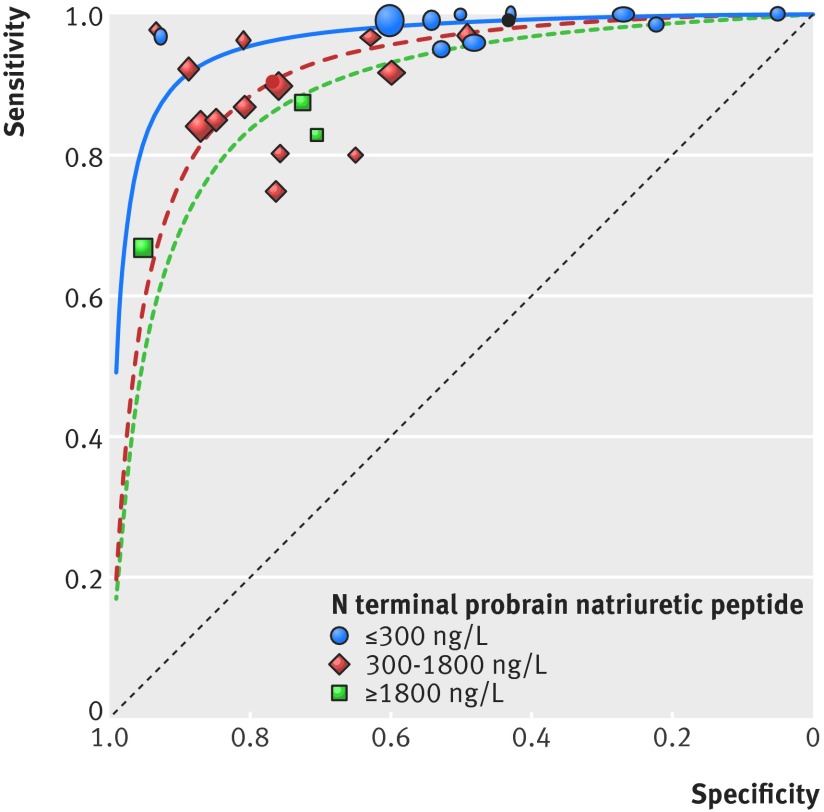
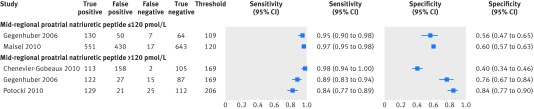
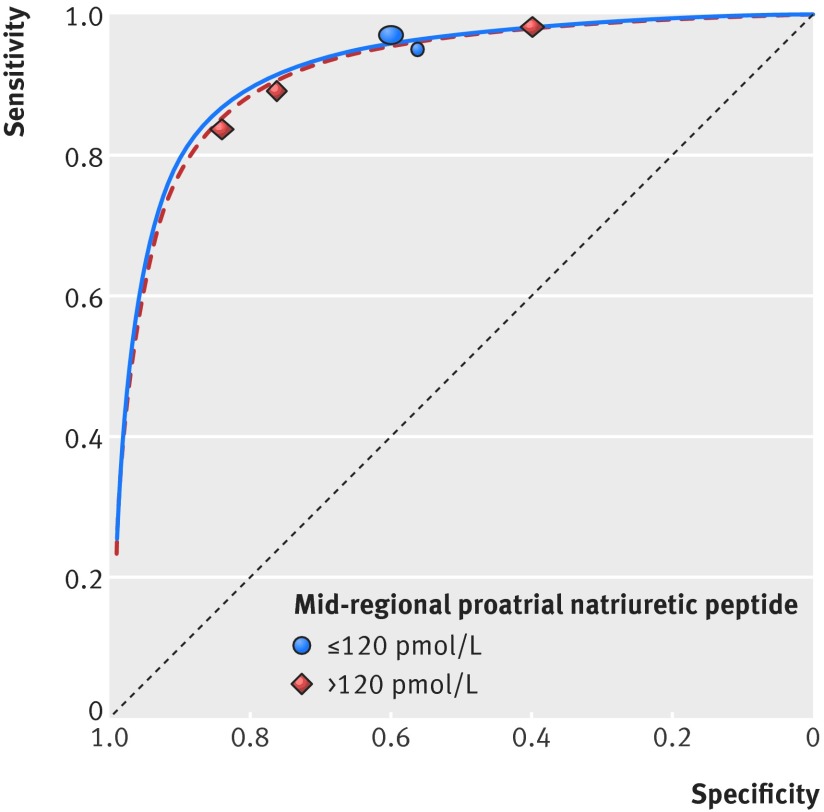
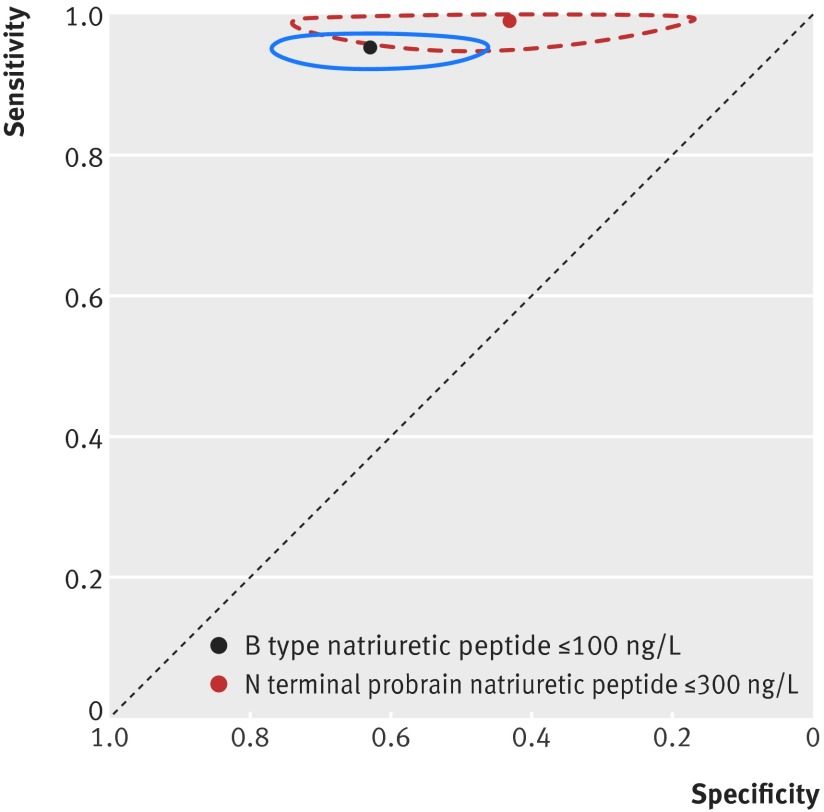
Results: 37 unique study cohorts described in 42 study reports were included, with a total of 48 test evaluations reporting 15 263 test results. At the lower recommended thresholds of 100 ng/L for B type natriuretic peptide and 300 ng/L for NTproBNP, the natriuretic peptides have sensitivities of 0.95 (95% confidence interval 0.93 to 0.96) and 0.99 (0.97 to 1.00) and negative predictive values of 0.94 (0.90 to 0.96) and 0.98 (0.89 to 1.0), respectively, for a diagnosis of acute heart failure. At the lower recommended threshold of 120 pmol/L, MRproANP has a sensitivity ranging from 0.95 (range 0.90-0.98) to 0.97 (0.95-0.98) and a negative predictive value ranging from 0.90 (0.80-0.96) to 0.97 (0.96-0.98). At higher thresholds the sensitivity declined progressively and specificity remained variable across the range of values. There was no statistically significant difference in diagnostic accuracy between plasma B type natriuretic peptide and NTproBNP.
Conclusions: At the rule-out thresholds recommended in the 2012 European Society of Cardiology guidelines for heart failure, plasma B type natriuretic peptide, NTproBNP, and MRproANP have excellent ability to exclude acute heart failure. Specificity is variable, and so imaging to confirm a diagnosis of heart failure is required. There is no statistical difference between the diagnostic accuracy of plasma B type natriuretic peptide and NTproBNP. Introduction of natriuretic peptide measurement in the investigation of patients with suspected acute heart failure has the potential to allow rapid and accurate exclusion of the diagnosis.
© Roberts et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner M, et al. ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines Circulation 2013;128:e240-327. - PubMed
-
- McMurray JJV, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2012;14:803-69. - PubMed
-
- Thygesen K1, Mair J, Mueller C, Huber K, Weber M, Plebani M, et al. Recommendations for the use of natriuretic peptides in acute cardiac care: a position statement from the Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care Eur Heart J 2012;33:2001-6. - PubMed
-
- Novielli N, Cooper NJ, Abrams KR, Sutton AJ. How is evidence on test performance synthesized for economic decision models of diagnostic tests? A systematic appraisal of Health Technology Assessments in the UK since 1997. Value Health 2010;13:952-7. - PubMed
-
- Fleischer D, Espiner EA, Yandle TG, Livesey JH, Billings J, Town I, et al. Rapid assay of plasma brain natriuretic peptide in the assessment of acute dyspnoea. N Z Med J 1997;110:71-4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous