

Primary cauda equina lymphoma: case report and literature review
- PMID: 25741044
- PMCID: PMC4345686
Primary cauda equina lymphoma: case report and literature review
Abstract
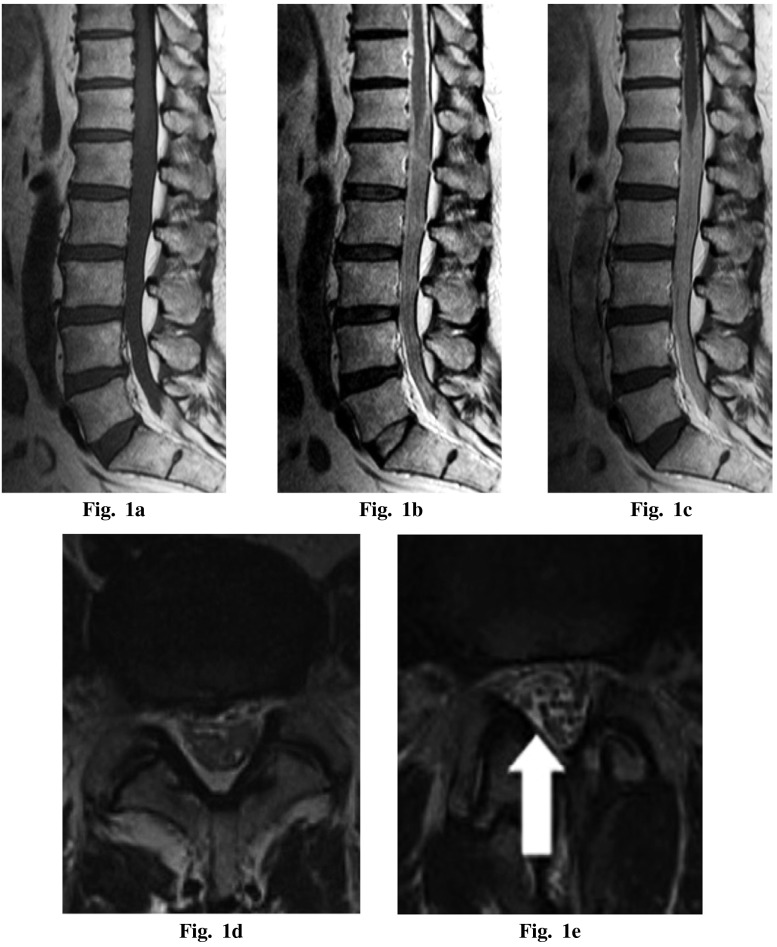
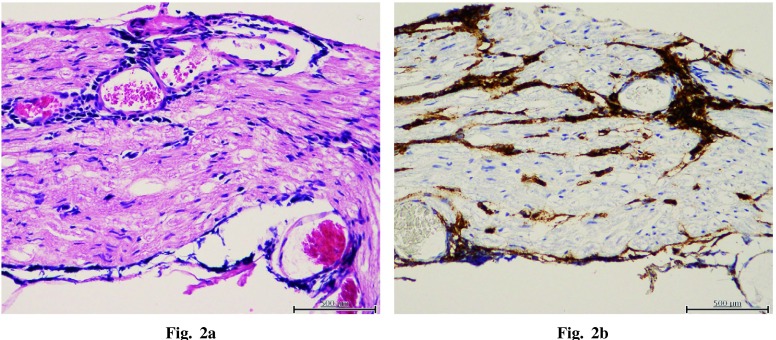
The central nervous system, in particular the spinal cord, is a rare site for primary lymphoma occurrence, with very few published cases. We report an extremely rare primary lymphoma in the cauda equina in a single case with literature review. An immunocompetent 59-year-old male, who complained of progressive low back and bilateral leg pain for 7 months, was studied. Magnetic resonance imaging (MRI) revealed an intradural space-occupying lesion from T12 to S1, poorly demarcated to the normal cauda equina. The intradural lesion showed T1 low intensity, T2 low isointensity, and marked homogeneous enhancement with gadolinium-diethylenetriaminepentaacetic acid on MRI. We performed spinal tap to obtain additional information about the intradural lesion. Large-sized atypical lymphoid cells were found during pathological examination. Fluorodeoxyglucose accumulation was found only in the lumbar area, which corresponded with the MRI findings, and the primary lymphoma site was defined as the cauda equina area. For further detailed pathological diagnosis, we performed surgical biopsy of the cauda equina. Morphological and immunohistochemical assessment made a diagnosis of diffuse large B-cell lymphoma of the cauda equina. The patient received radiotherapy to the lumbosacral area (50 Gy) and methotrexate (MTX) therapy after surgery. The patient was able to walk without help after the therapies. Follow-up MRI performed 1 year after biopsy showed remission of the lesion. MRI and spinal tap were effective tools for the early definitive diagnosis of cauda equina lymphoma. Combined treatment with radiotherapy and MTX should be performed as early as possible.
Keywords: B-cell lymphoma; cauda equina; primary lymphoma.
Figures
Similar articles
-
Primary cauda equina lymphoma diagnosed by nerve biopsy: A case report and literature review.Oncol Lett. 2018 Jul;16(1):623-631. doi: 10.3892/ol.2018.8629. Epub 2018 May 4. Oncol Lett. 2018. PMID: 29928449 Free PMC article.
-
Primary NK/T-cell lymphoma of the cauda equina: a case report and literature review.Spine (Phila Pa 1976). 2009 Nov 15;34(24):E882-5. doi: 10.1097/BRS.0b013e3181b29de6. Spine (Phila Pa 1976). 2009. PMID: 19910757 Review.
-
Primary Malignant Lymphoma of the Cauda Equina Diagnosed after Decompression for Lumbar Spinal Stenosis: A Case Report.Tohoku J Exp Med. 2023 Aug 23;260(4):341-346. doi: 10.1620/tjem.2023.J047. Epub 2023 Jun 8. Tohoku J Exp Med. 2023. PMID: 37286520
-
MR Imaging Characteristics of Primary T-Cell Lymphoma of the Cauda Equina: A Case Report and Literature Review.Taehan Yongsang Uihakhoe Chi. 2021 Nov;82(6):1613-1618. doi: 10.3348/jksr.2020.0195. Epub 2021 Oct 18. Taehan Yongsang Uihakhoe Chi. 2021. PMID: 36238886 Free PMC article.
-
Primary Cauda Equina Lymphoma Mimicking Meningioma.J Clin Med. 2024 Aug 22;13(16):4959. doi: 10.3390/jcm13164959. J Clin Med. 2024. PMID: 39201102 Free PMC article. Review.
Cited by
-
Primary cauda equina lymphoma diagnosed by nerve biopsy: A case report and literature review.Oncol Lett. 2018 Jul;16(1):623-631. doi: 10.3892/ol.2018.8629. Epub 2018 May 4. Oncol Lett. 2018. PMID: 29928449 Free PMC article.
-
Primary Cauda Equina Lymphoma Treated with CNS-Centric Approach: A Case Report and Literature Review.J Blood Med. 2021 Jul 21;12:645-652. doi: 10.2147/JBM.S325264. eCollection 2021. J Blood Med. 2021. PMID: 34321945 Free PMC article.
-
Non-Hodgkin Lymphoma of Cauda Equina: A Diagnostic Conundrum: Case Report.Adv Biomed Res. 2023 Apr 25;12:95. doi: 10.4103/abr.abr_36_21. eCollection 2023. Adv Biomed Res. 2023. PMID: 37288018 Free PMC article.
-
F-18 Fluorodeoxyglucose Positron Emission Tomography Computed Tomography Findings in an Interesting Case of Primary Cauda Equina Lymphoma with Literature Review.Indian J Nucl Med. 2021 Oct-Dec;36(4):425-428. doi: 10.4103/ijnm.ijnm_75_21. Epub 2021 Dec 15. Indian J Nucl Med. 2021. PMID: 35125761 Free PMC article.
-
Unusual cauda equina syndrome due to multifocal ependymoma infiltrated by lymphoma.J Spine Surg. 2017 Dec;3(4):697-701. doi: 10.21037/jss.2017.10.02. J Spine Surg. 2017. PMID: 29354750 Free PMC article.
References
-
- Eichler AF, Batchelor TT. Primary central nervous system lymphoma: presentation, diagnosis and staging. Neurosurg Focus, 2006; 21: E15. - PubMed
-
- Hochberg FH, Miller DC. Primary central nervous system lymphoma. J Neurosurg, 1988; 68: 835–853. - PubMed
-
- Ferreri AJ, Blay JY, Reni M, Pasini F, Spina M, Ambrosetti A, Calderoni A, Rossi A, Vavassori V, Conconi A, Devizzi L, Berger F, Ponzoni M, Borisch B, Tinguely M, Cerati M, Milani M, Orvieto E, Sanchez J, Chevreau C, Dell’Oro S, Zucca E, Cavalli F. Prognostic scoring system for primary CNS lymphomas: the International Extranodal Lymphoma Study Group experience. J Clin Oncol, 2003; 21: 266–272. - PubMed
-
- Iwamoto FM, DeAngelis LM. An update on primary central nervous system lymphoma. Hematol Oncol Clin North Am, 2006; 20: 1267–1285. - PubMed
-
- Lukes RJ, Collins RD. Immunologic characterization of human malignant lymphomas. Cancer, 1974; 34: 1488–1503. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous