

Hepatobiliary contrast agents: differential diagnosis of focal hepatic lesions, pitfalls and other indications
- PMID: 25741105
- PMCID: PMC4341386
- DOI: 10.1590/0100-3984.2013.1867
Hepatobiliary contrast agents: differential diagnosis of focal hepatic lesions, pitfalls and other indications
Abstract
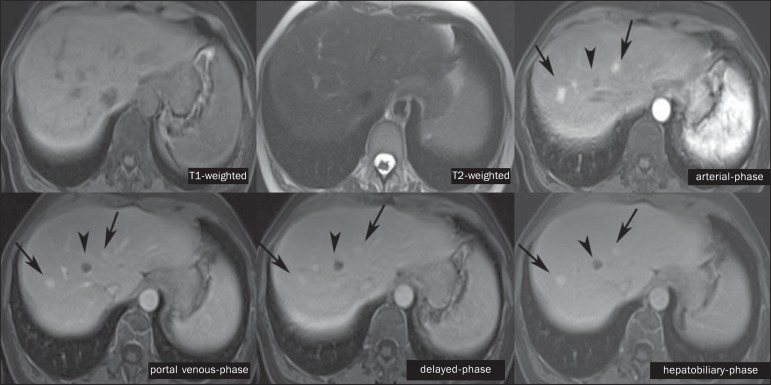
The characterization of focal liver lesions is very important. Magnetic resonance imaging is considered the best imaging method for evaluating such lesions, but does not allow for the diagnosis in all cases. The use of hepatobiliary contrast agents increases the diagnostic accuracy of magnetic resonance imaging and reduces the number of non-specific liver lesions. The main indications for the method include: differentiation between focal nodular hyperplasia and adenoma; characterization of hepatocellular carcinomas in cirrhotic patients; detection of small liver metastases; evaluation of biliary anatomy; and characterization of postoperative biliary fistulas. The use of hepatobiliary contrast agents may reduce the need for invasive diagnostic procedures and further investigations with other imaging methods, besides the need for imaging follow-up.
A caracterização das lesões hepáticas focais é muito importante. A ressonância magnética é considerada o melhor método de imagem para a avaliação destas lesões, mas não permite o diagnóstico em todos os casos. Os contrastes hepatobiliares aumentam a acurácia diagnóstica da ressonância magnética e diminuem o número de lesões hepáticas indefinidas. Suas principais indicações são a diferenciação entre hiperplasia nodular focal e adenoma, caracterização de carcinoma hepatocelular em pacientes cirróticos, detecção de metástases hepáticas pequenas, avaliação da anatomia biliar e identificação de fístulas biliares pós-operatórias. A utilização dos contrastes hepatobiliares pode reduzir a necessidade de procedimentos diagnósticos invasivos e de avaliação complementar por outros exames de imagem, além de diminuir a necessidade de exames de acompanhamento.
Keywords: Focal hepatic lesions; Hepatobiliary contrast; Magnetic resonance imaging.
Figures



Similar articles
-
[Gd-EOB-DTPA-enhanced magnetic resonance imaging: differentiation between focal nodular hyperplasia and hepatocellular adenoma].Acta Med Port. 2011 Dec;24 Suppl 2:531-8. Epub 2011 Dec 31. Acta Med Port. 2011. PMID: 22849944 Portuguese.
-
An update on clinical applications of hepatospecific contrast media in magnetic resonance imaging of liver parenchyma.Eur Rev Med Pharmacol Sci. 2016 Jun;20(12):2515-25. Eur Rev Med Pharmacol Sci. 2016. PMID: 27383300
-
Spectrum of liver lesions hyperintense on hepatobiliary phase: an approach by clinical setting.Insights Imaging. 2021 Jan 12;12(1):8. doi: 10.1186/s13244-020-00928-w. Insights Imaging. 2021. PMID: 33432491 Free PMC article. Review.
-
Dual contrast liver MRI: a pictorial illustration.Abdom Radiol (NY). 2021 Oct;46(10):4588-4600. doi: 10.1007/s00261-021-03129-1. Epub 2021 Jun 2. Abdom Radiol (NY). 2021. PMID: 34076723 Review.
-
Characterization of focal hepatic lesions with ferumoxides-enhanced T2-weighted MR imaging.AJR Am J Roentgenol. 2000 Jul;175(1):159-63. doi: 10.2214/ajr.175.1.1750159. AJR Am J Roentgenol. 2000. PMID: 10882267
Cited by
-
Evaluating Pre-Interventional Administration of a Liver-Specific Contrast Agent During MRI-Guided Thermal Ablation of Malignant Liver Lesions.Cancers (Basel). 2025 Apr 9;17(8):1264. doi: 10.3390/cancers17081264. Cancers (Basel). 2025. PMID: 40282440 Free PMC article.
-
Imaging Diagnosis of Hepatocellular Carcinoma: A State-of-the-Art Review.Diagnostics (Basel). 2023 Feb 8;13(4):625. doi: 10.3390/diagnostics13040625. Diagnostics (Basel). 2023. PMID: 36832113 Free PMC article. Review.
-
Can gadoxetic acid-enhanced magnetic resonance imaging be used to avoid liver biopsy in patients with nonalcoholic fatty liver disease?World J Hepatol. 2020 Sep 27;12(9):661-671. doi: 10.4254/wjh.v12.i9.661. World J Hepatol. 2020. PMID: 33033571 Free PMC article.
-
Morphological, dynamic and functional characteristics of liver pseudolesions and benign lesions.Radiol Med. 2022 Feb;127(2):129-144. doi: 10.1007/s11547-022-01449-w. Epub 2022 Jan 13. Radiol Med. 2022. PMID: 35028886 Review.
-
Imaging evaluation in metabolic syndrome: beyond steatosis.Radiol Bras. 2016 Jan-Feb;49(1):V-VI. doi: 10.1590/0100-3984.2016.49.1e1. Radiol Bras. 2016. PMID: 26929471 Free PMC article. No abstract available.
References
-
- Goodwin MD, Dobson JE, Sirlin CB, et al. Diagnostic challenges and pitfalls in MR imaging with hepatocyte-specific contrast agents. Radiographics. 2011;31:1547–1568. - PubMed
-
- Ba-Ssalamah A, Uffmann M, Saini S, et al. Clinical value of MRI liver-specific contrast agents: a tailored examination for a confident non-invasive diagnosis of focal liver lesions. Eur Radiol. 2009;19:342–357. - PubMed
-
- Hammerstingl R, Zangos S, Schwarz W, et al. Contrast-enhanced MRI of focal liver tumors using a hepatobiliary MR contrast agent: detection and differential diagnosis using Gd-EOB-DTPA-enhanced versus Gd-DTPA-enhanced MRI in the same patient. Acad Radiol. 2002;9(Suppl 1):S119–S120. - PubMed
-
- Seale MK, Catalano OA, Saini S, et al. Hepatobiliary-specific MR contrast agents: role in imaging the liver and biliary tree. Radiographics. 2009;29:1725–1748. - PubMed
-
- Lee NK, Kim S, Lee JW, et al. Biliary MR imaging with Gd-EOBDTPA and its clinical applications. Radiographics. 2009;29:1707–1724. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources