

Clinical observations on the treatment of prolapsing hemorrhoids with tissue selecting therapy
- PMID: 25741159
- PMCID: PMC4342928
- DOI: 10.3748/wjg.v21.i8.2490
Clinical observations on the treatment of prolapsing hemorrhoids with tissue selecting therapy
Abstract
Aim: To compare the effects and postoperative complications between tissue selecting therapy stapler (TST) and Milligan-Morgan hemorrhoidectomy (M-M).
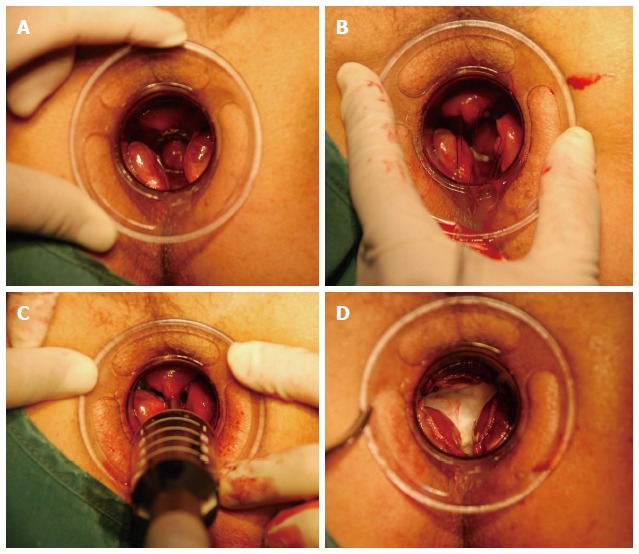
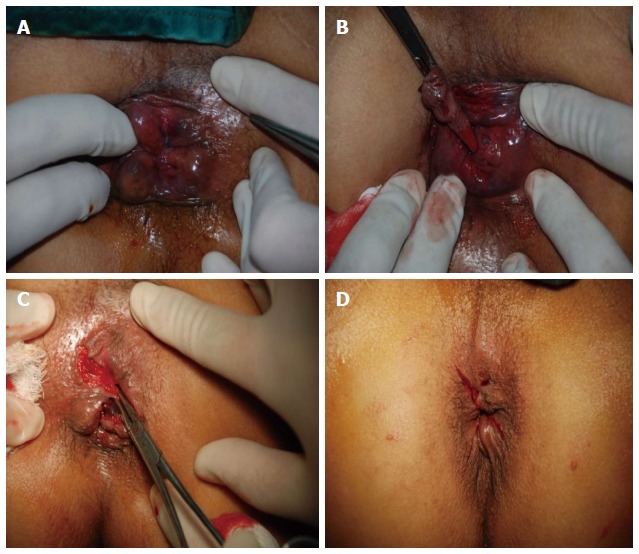
Methods: Four hundred and eighty patients with severe prolapsing hemorrhoids, who were admitted to the Shenyang Coloproctology Hospital between 2009 and 2012, were randomly divided into observation (n=240) and control (n=240) groups. Hemorrhoidectomies were performed with TST in the observation group and with the M-M technique in the control group. The therapeutic effects, operation security, and postoperative complications in the two groups were compared. The immediate and long-term complications were assessed according to corresponding criteria. Pain was assessed on a visual analogue scale. The efficacy was assessed by specialized criteria. The follow-up was conducted one year after the operation.
Results: The total effective rates of the observation and control groups were 99.5% (217/218) and 98.6% (218/221) respectively; the difference was not statistically significant (P=0.322). Their were significant differences between observation and control groups in intraoperative blood loss (5.07±1.14 vs 2.45±0.57, P=0.000), pain (12 h after the surgery: 5.08±1.62 vs 7.19±2.01, P=0.000; at first dressing change: 2.64±0.87 vs 4.34±1.15, P=0.000; first defecation: 3.91±1.47 vs 5.63±1.98, P=0.001), urine retention (n=22 vs n=47, P=0.001), anal pendant expansion after the surgery (2.35±0.56 vs 5.16±1.42, P=0.000), operation time (18.3±5.6 min vs 29.5±8.2 min, P=0.000), and the length of hospital stay (5.3±0.6 d vs 11.4±1.8 d, P=0.000). Moreover TST showed significant reductions compared to M-M in the rates of long-term complications such as fecal incontinence (n=3 vs n=16, P=0.003), difficult bowel movement (n=1 vs n=9, P=0.011), intractable pain (n=2 vs n=12, P=0.007), and anal discharge (n=3 vs n=23, P=0.000).
Conclusion: TST for severe prolapsing hemorrhoids is a satisfactory technique for more rapid recovery, lower complication rates, and higher operation security.
Keywords: Complication rate; Milligan-Morgan hemorrhoidectomy; Operation security; Severe prolapsing hemorrhoids; Tissue selecting therapy stapler.
Figures
Similar articles
-
A prospective randomized controlled trial evaluating the short-term outcomes of transanal hemorrhoidal dearterialization versus tissue-selecting technique.Tech Coloproctol. 2017 Sep;21(9):737-743. doi: 10.1007/s10151-017-1669-x. Epub 2017 Sep 20. Tech Coloproctol. 2017. PMID: 28932913 Clinical Trial.
-
Procedure for prolapse and hemorrhoids vs traditional surgery for outlet obstructive constipation.World J Gastroenterol. 2015 Jul 14;21(26):8178-83. doi: 10.3748/wjg.v21.i26.8178. World J Gastroenterol. 2015. PMID: 26185392 Free PMC article. Clinical Trial.
-
Procedure for prolapse and hemorrhoids (PPH) with low rectal anastomosis using a PPH 03 stapler: low rate of recurrence and postoperative complications.Int J Colorectal Dis. 2017 Dec;32(12):1687-1692. doi: 10.1007/s00384-017-2908-3. Epub 2017 Sep 27. Int J Colorectal Dis. 2017. PMID: 28956135
-
Network meta-analysis of randomized controlled trials comparing the procedure for prolapse and hemorrhoids, Milligan-Morgan hemorrhoidectomy and tissue-selecting therapy stapler in the treatment of grade III and IV internal hemorrhoids(Meta-analysis).Int J Surg. 2020 Feb;74:53-60. doi: 10.1016/j.ijsu.2019.12.027. Epub 2019 Dec 27. Int J Surg. 2020. PMID: 31887419 Review.
-
[Which surgical technique for stage IV haemorrhoids?].Ann Chir. 2003 Nov;128(9):616-8. doi: 10.1016/j.anchir.2003.09.013. Ann Chir. 2003. PMID: 14659616 Review. French. No abstract available.
Cited by
-
Treatment of hemorrhoids with individualized homeopathy: An open observational pilot study.J Intercult Ethnopharmacol. 2016 Jun 25;5(4):335-342. doi: 10.5455/jice.20160608030224. eCollection 2016 Sep-Dec. J Intercult Ethnopharmacol. 2016. PMID: 27757262 Free PMC article.
-
A prospective randomized controlled trial evaluating the short-term outcomes of transanal hemorrhoidal dearterialization versus tissue-selecting technique.Tech Coloproctol. 2017 Sep;21(9):737-743. doi: 10.1007/s10151-017-1669-x. Epub 2017 Sep 20. Tech Coloproctol. 2017. PMID: 28932913 Clinical Trial.
-
Evaluation of the clinical efficacy and safety of TST33 mega hemorrhoidectomy for severe prolapsed hemorrhoids.World J Clin Cases. 2022 Jun 26;10(18):6060-6068. doi: 10.12998/wjcc.v10.i18.6060. World J Clin Cases. 2022. PMID: 35949822 Free PMC article.
-
A novel technique for the treatment of stages III to IV hemorrhoids: Homemade anal cushion suspension clamp combined with harmonic scalpel.Medicine (Baltimore). 2017 Jun;96(26):e7309. doi: 10.1097/MD.0000000000007309. Medicine (Baltimore). 2017. PMID: 28658138 Free PMC article.
-
The comparison of an accessible C-shaped partial stapled hemorrhoidopexy (C-PSH) versus circular stapled hemorrhoidopexy (CSH) in patients with grade IV hemorrhoids: a retrospective cohort study.BMC Gastroenterol. 2023 Dec 16;23(1):443. doi: 10.1186/s12876-023-03062-1. BMC Gastroenterol. 2023. PMID: 38104065 Free PMC article.
References
-
- Argov S, Levandovsky O, Yarhi D. Milligan-Morgan hemorrhoidectomy under local anesthesia - an old operation that stood the test of time. A single-team experience with 2,280 operations. Int J Colorectal Dis. 2012;27:981–985. - PubMed
-
- Longo A. Treatment of hemorrhoidal disease by reduction of mucosa and hemorrhoidal prolapse with circular suturing device: a new procedure. In: Proceedings of the 6th World Congress of Endoscopic Surgery., editor. Bologna: Munduzzi; 1988. pp. 777–784.
-
- Fueglistaler P, Guenin MO, Montali I, Kern B, Peterli R, von Flüe M, Ackermann C. Long-term results after stapled hemorrhoidopexy: high patient satisfaction despite frequent postoperative symptoms. Dis Colon Rectum. 2007;50:204–212. - PubMed
-
- Lin HC, He QL, Ren DL, Peng H, Xie SK, Su D, Wang XX. Partial stapled hemorrhoidopexy: a minimally invasive technique for hemorrhoids. Surg Today. 2012;42:868–875. - PubMed
-
- Khubchandani IT. H.-C. Lin, D.-L. Ren, Q.-L. He, H. Peng, S.-K. Xie, D. Su, X.-X. Wang: Partial stapled hemorrhoidopexy versus circular stapled hemorrhoidopexy for grade III-IV prolapsing hemorrhoids: a two-year prospective controlled study. Tech Coloproctol. 2012;16:345; discussion 347–348. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
