

Coronary artery imaging in children
- PMID: 25741188
- PMCID: PMC4347262
- DOI: 10.3348/kjr.2015.16.2.239
Coronary artery imaging in children
Abstract
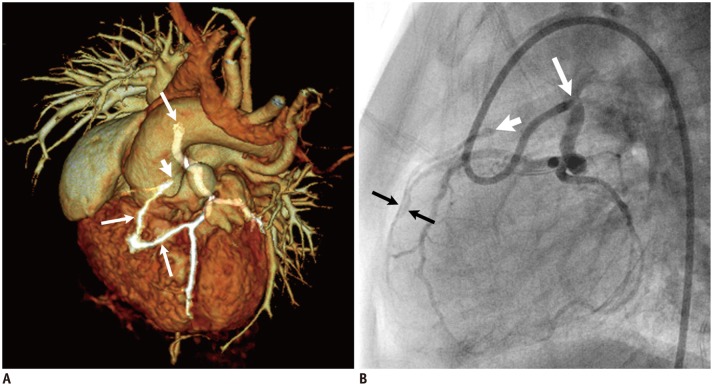
Coronary artery problems in children usually have a significant impact on both short-term and long-term outcomes. Early and accurate diagnosis, therefore, is crucial but technically challenging due to the small size of the coronary artery, high heart rates, and limited cooperation of children. Coronary artery visibility on CT and MRI in children is considerably improved with recent technical advancements. Consequently, CT and MRI are increasingly used for evaluating various congenital and acquired coronary artery abnormalities in children, such as coronary artery anomalies, aberrant coronary artery anatomy specific to congenital heart disease, Kawasaki disease, Williams syndrome, and cardiac allograft vasculopathy.
Keywords: CT; Catheter angiography; Coronary artery; Echocardiography; Infants and children; MRI.
Figures


References
-
- Lederlin M, Thambo JB, Latrabe V, Corneloup O, Cochet H, Montaudon M, et al. Coronary imaging techniques with emphasis on CT and MRI. Pediatr Radiol. 2011;41:1516–1525. - PubMed
-
- Tang L, Merkle N, Schär M, Korosoglou G, Solaiyappan M, Hombach V, et al. Volume-targeted and whole-heart coronary magnetic resonance angiography using an intravascular contrast agent. J Magn Reson Imaging. 2009;30:1191–1196. - PubMed
-
- Vranicar M, Hirsch R, Canter CE, Balzer DT. Selective coronary angiography in pediatric patients. Pediatr Cardiol. 2000;21:285–288. - PubMed
-
- Attili A, Hensley AK, Jones FD, Grabham J, DiSessa TG. Echocardiography and coronary CT angiography imaging of variations in coronary anatomy and coronary abnormalities in athletic children: detection of coronary abnormalities that create a risk for sudden death. Echocardiography. 2013;30:225–233. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
