

A multi-institutional experience in pediatric high-grade glioma
- PMID: 25741472
- PMCID: PMC4332307
- DOI: 10.3389/fonc.2015.00028
A multi-institutional experience in pediatric high-grade glioma
Abstract
Introduction: Pediatric high-grade gliomas are rare tumors with poor outcomes and incompletely defined management. We conducted a multi-institutional retrospective study to evaluate association of clinical, pathologic, and treatment characteristics with outcomes.
Materials and methods: Fifty-one patients treated from 1984 to 2008 at the Ohio State University or University of Michigan were included. Histologic subgroups were compared. Log-rank and stepwise Cox proportional hazard modeling were used to analyze progression-free survival (PFS) and overall survival (OS) within the whole group, grade III subgroup, grade IV subgroup, and sub-total resection/biopsy subgroup.
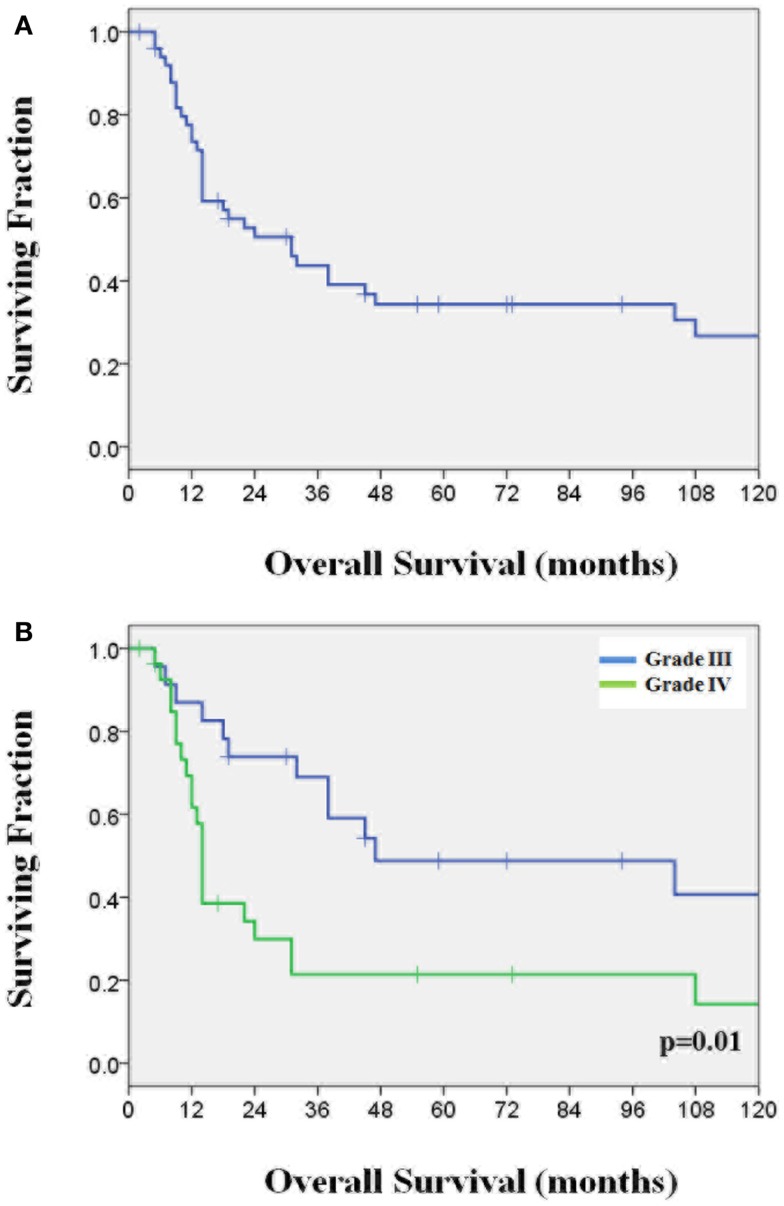
Results: Median OS was 27.6 months. Grade III histology, complete tumor resection, and cerebral tumor location correlated with improved PFS and OS. Temozolomide use and chemotherapy after radiotherapy or chemoradiation (CRT) were associated with better PFS while seizure at presentation was associated with better OS. In multivariate analysis, complete resection and chemotherapy following radiotherapy or CRT were independent predictors for improved PFS and OS. For grade III and IV subgroups, complete resection was associated with improved OS (grade III) and seizure presentation was associated with improved OS (grade IV). In the incompletely resection subgroup, temozolomide use and concurrent CRT independently correlated with improved PFS, while higher radiation dose (≥59.4 Gy) and adjuvant chemotherapy were independently associated with improved OS.
Discussion: Total resection and receiving chemotherapy adjuvant to radiation or CRT are most closely associated with improved PFS and OS. For higher risk incompletely resected patients, temozolomide use and treatment intensification with concurrent CRT, adjuvant chemotherapy, and higher radiation dose were associated with improved outcomes.
Keywords: chemotherapy; glioblastoma; high-grade glioma; pediatric cancer; radiation therapy.
Figures
Similar articles
-
Prognostic factors effective on survival of patients with glioblastoma: Anadolu Medical Center experience.Indian J Cancer. 2016 Jul-Sep;53(3):382-386. doi: 10.4103/0019-509X.200664. Indian J Cancer. 2016. PMID: 28244465
-
The impact of adjuvant therapy for patients with high-risk diffuse WHO grade II glioma.J Neurooncol. 2017 Dec;135(3):535-543. doi: 10.1007/s11060-017-2599-1. Epub 2017 Aug 23. J Neurooncol. 2017. PMID: 28836106
-
Prospective clinical trials of intracranial low-grade glioma in adults and children.Neuro Oncol. 2003 Jul;5(3):153-60. doi: 10.1215/S1152851702000601. Neuro Oncol. 2003. PMID: 12816721 Free PMC article. Review.
-
Radiotherapy versus radiotherapy combined with temozolomide in high-risk low-grade gliomas after surgery: study protocol for a randomized controlled clinical trial.Trials. 2019 Nov 21;20(1):641. doi: 10.1186/s13063-019-3741-5. Trials. 2019. PMID: 31752981 Free PMC article.
-
Supratentorial hemispheric ependymomas: an analysis of 109 adults for survival and prognostic factors.J Neurosurg. 2016 Aug;125(2):410-8. doi: 10.3171/2015.7.JNS151187. Epub 2016 Jan 8. J Neurosurg. 2016. PMID: 26745489 Review.
Cited by
-
Prognostic factors for pediatric, adolescent, and young adult patients with non-DIPG grade 4 gliomas: a contemporary pooled institutional experience.J Neurooncol. 2023 Jul;163(3):717-726. doi: 10.1007/s11060-023-04386-4. Epub 2023 Jul 13. J Neurooncol. 2023. PMID: 37440097 Free PMC article.
-
High-Grade Gliomas in Children-A Multi-Institutional Polish Study.Cancers (Basel). 2021 Apr 24;13(9):2062. doi: 10.3390/cancers13092062. Cancers (Basel). 2021. PMID: 33923337 Free PMC article.
-
Multicentric glioblastoma in a 4-year-old female patient: A case report.Mol Clin Oncol. 2021 May;14(5):90. doi: 10.3892/mco.2021.2252. Epub 2021 Mar 5. Mol Clin Oncol. 2021. PMID: 33767859 Free PMC article.
-
Does the interval from tumour surgery to radiotherapy influence survival in paediatric high grade glioma?Strahlenther Onkol. 2018 Jun;194(6):552-559. doi: 10.1007/s00066-018-1260-z. Epub 2018 Jan 18. Strahlenther Onkol. 2018. PMID: 29349602 Free PMC article.
-
Evaluating extent of resection in pediatric glioblastoma: a multiple propensity score-adjusted population-based analysis.Childs Nerv Syst. 2016 Mar;32(3):493-503. doi: 10.1007/s00381-015-3006-x. Epub 2016 Jan 15. Childs Nerv Syst. 2016. PMID: 26767842
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials