

Severe root resorption resulting from orthodontic treatment: prevalence and risk factors
- PMID: 25741825
- PMCID: PMC4373016
- DOI: 10.1590/2176-9451.20.1.052-058.oar
Severe root resorption resulting from orthodontic treatment: prevalence and risk factors
Abstract
Objective: To assess the prevalence of severe external root resorption and its potential risk factors resulting from orthodontic treatment.
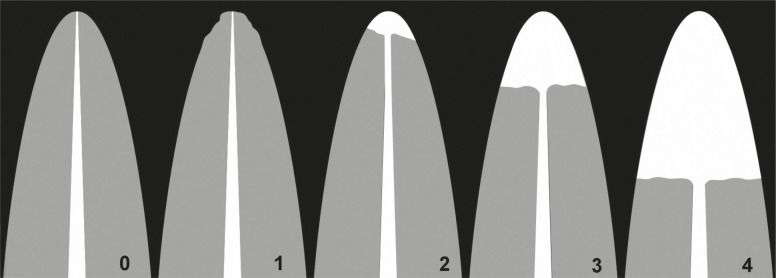
Methods: A randomly selected sample was used. It comprised conventional periapical radiographs taken in the same radiology center for maxillary and mandibular incisors before and after active orthodontic treatment of 129 patients, males and females, treated by means of the Standard Edgewise technique. Two examiners measured and defined root resorption according to the index proposed by Levander et al. The degree of external apical root resorption was registered defining resorption in four degrees of severity. To assess intra and inter-rater reproducibility, kappa coefficient was used. Chi-square test was used to assess the relationship between the amount of root resorption and patient's sex, dental arch (maxillary or mandibular), treatment with or without extractions, treatment duration, root apex stage (open or closed), root shape, as well as overjet and overbite at treatment onset.
Results: Maxillary central incisors had the highest percentage of severe root resorption, followed by maxillary lateral incisors and mandibular lateral incisors. Out of 959 teeth, 28 (2.9%) presented severe root resorption. The following risk factors were observed: anterior maxillary teeth, overjet greater than or equal to 5 mm at treatment onset, treatment with extractions, prolonged therapy, and degree of apex formation at treatment onset.
Conclusion: This study showed that care must be taken in orthodontic treatment involving extractions, great retraction of maxillary incisors, prolonged therapy, and/or completely formed apex at orthodontic treatment onset.
OBJETIVO:: avaliar a prevalência de reabsorções radiculares externas severas e identificar prováveis fatores de risco decorrentes do tratamento ortodôntico.
MÉTODOS:: utilizou-se uma amostra selecionada aleatoriamente, composta de radiografias periapicais de incisivos superiores e inferiores, obtidas no mesmo centro radiológico, de pré- e pós-tratamento ortodôntico ativo, de 129 pacientes, de ambos os sexos, tratados por meio da técnica Edgewise Standard. Dois examinadores mensuraram e definiram a reabsorção radicular de acordo com índice proposto por Levander et al., e o grau de reabsorção foi registrado, definindo a reabsorção em quatro graus de severidade. Para avaliar a reprodutibilidade intra- e interexaminadores, adotou-se o índice de coeficiente kappa ponderado. O teste chi-quadrado (χ2) foi adotado para avaliar a relação entre a quantidade de reabsorção radicular e o sexo dos pacientes, arcada dentária (superior ou inferior), tratamentos com ou sem extrações, duração do tratamento, forma radicular, estágio do ápice radicular (aberto ou fechado), overjet e overbite no início do tratamento.
RESULTADOS:: os incisivos centrais superiores apresentaram a maior porcentagem de reabsorção radicular severa, seguidos dos incisivos laterais superiores e dos incisivos laterais inferiores. Entre 959 dentes avaliados, 28 (2,9%) apresentaram reabsorção radicular severa. Os fatores de risco relacionados foram: dentes localizados na região anterossuperior, overjet maior ou igual a 5mm ao início do tratamento, tratamentos envolvendo extrações dentárias, tempo prolongado de terapia e formação radicular completa à época do início do tratamento ortodôntico.
CONCLUSÃO:: o estudo demonstrou que cuidados devem ser tomados em tratamentos ortodônticos envolvendo extrações, com grande retração de incisivos superiores, tratamentos prolongados e/ou ápice radicular completamente formado no início da terapia ortodôntica.
Figures
References
-
- Artun J, Van't Hullenaar R, Doppel D, Kuijpers-Jagtman AM. Identification of orthodontic patients at risk of severe apical root resorption. Am J Orthod Dentofacial Orthop. 2009;135(4):448–455. - PubMed
-
- Bartley N, Türk T, Colak C, Elekdaq-Türk S, Jones A, Petocz P, et al. Physical properties of root cementum: Part 17. Root resorption after the application of 2.50 and 150 of buccal root torque for 4 weeks: a micro computed tomography study. Am J Orthod Dentofacial Orthop. 2011;139(4):e353–e360. - PubMed
-
- Brin I, Tulloch JC, Koroluk L, Philips C. External apical root resorption in Class II malocclusion: a retrospective review of 1- versus 2-phase treatment. Am J Orthod Dentofacial Orthop. 2003;124(2):151–156. - PubMed
-
- Montenegro VJ, Jones A, Petocz P, Gonzales C, Darendeliler MA. Physical properties of root cementum: Part 22. Root resorption after the application of light and heavy extrusive orthodontic forces: a microcomputed tomography study Am J Orthod Dentofacial Orthop. 2012;141(1):e1–e9. - PubMed
-
- Sameshima GT, Sinclair PM. Predicting and preventing root resorption: Part I. Diagnostic factors. Am J Orthod Dentofacial Orthop. 2001;119(5):505–510. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
