

Let's Talk Critical. Development and Evaluation of a Communication Skills Training Program for Critical Care Fellows
- PMID: 25741996
- PMCID: PMC4418330
- DOI: 10.1513/AnnalsATS.201501-040OC
Let's Talk Critical. Development and Evaluation of a Communication Skills Training Program for Critical Care Fellows
Abstract
Rationale: Although expert communication between intensive care unit clinicians with patients or surrogates improves patient- and family-centered outcomes, fellows in critical care medicine do not feel adequately trained to conduct family meetings.
Objectives: We aimed to develop, implement, and evaluate a communication skills program that could be easily integrated into a U.S. critical care fellowship.
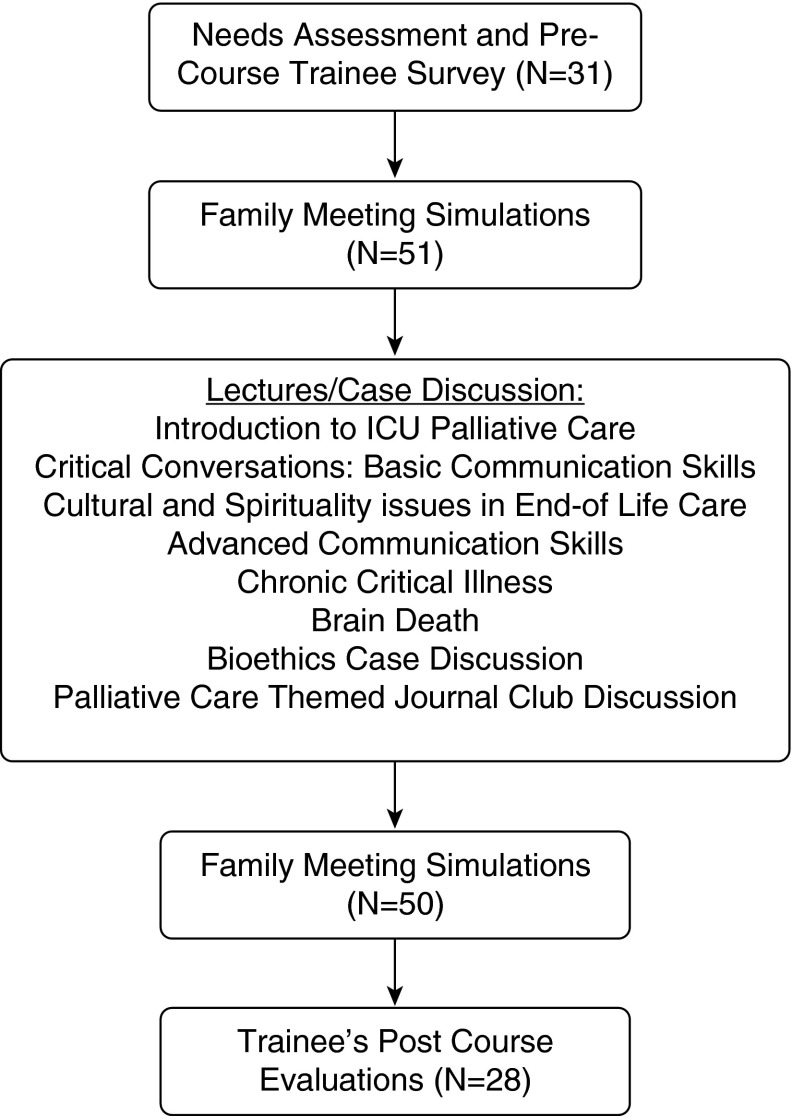
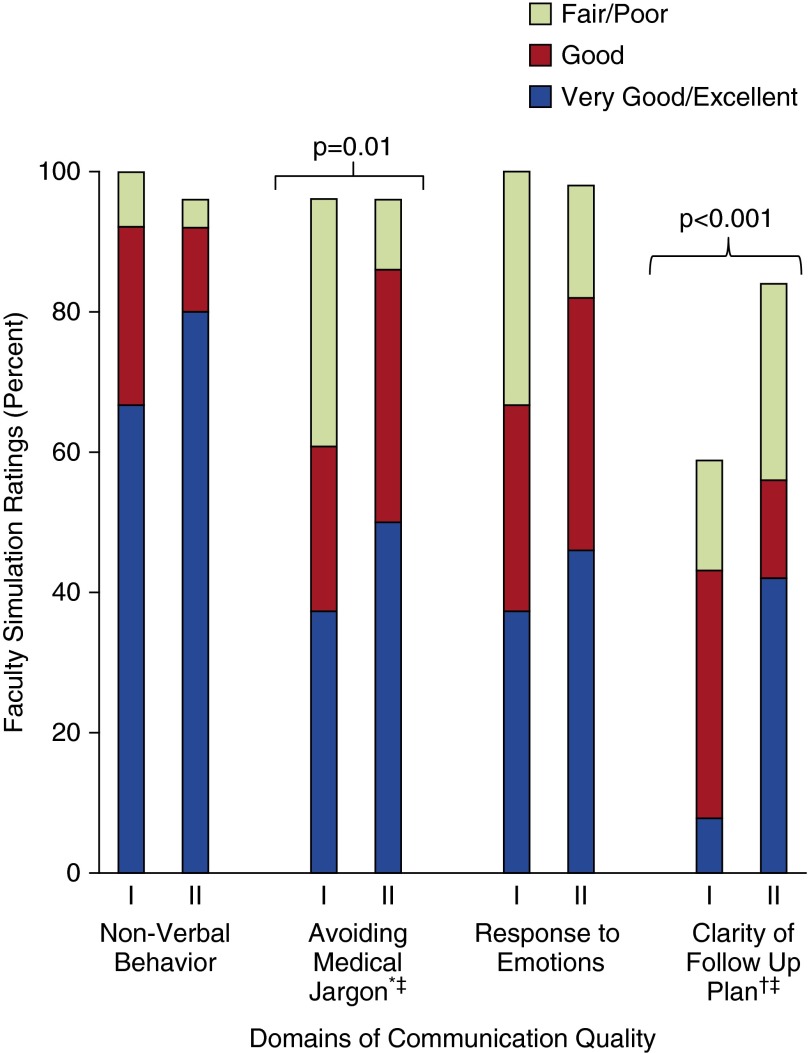
Methods: We developed four simulation cases that provided communication challenges that critical care fellows commonly face. For each case, we developed a list of directly observable tasks that could be used by faculty to evaluate fellows during each simulation. We developed a didactic curriculum of lectures/case discussions on topics related to palliative care, end-of-life care, communication skills, and bioethics; this month-long curriculum began and ended with the fellows leading family meetings in up to two simulated cases with direct observation by faculty who were not blinded to the timing of the simulation. Our primary measures of effectiveness were the fellows' self-reported change in comfort with leading family meetings after the program was completed and the quality of the communication as measured by the faculty evaluators during the family meeting simulations at the end of the month.
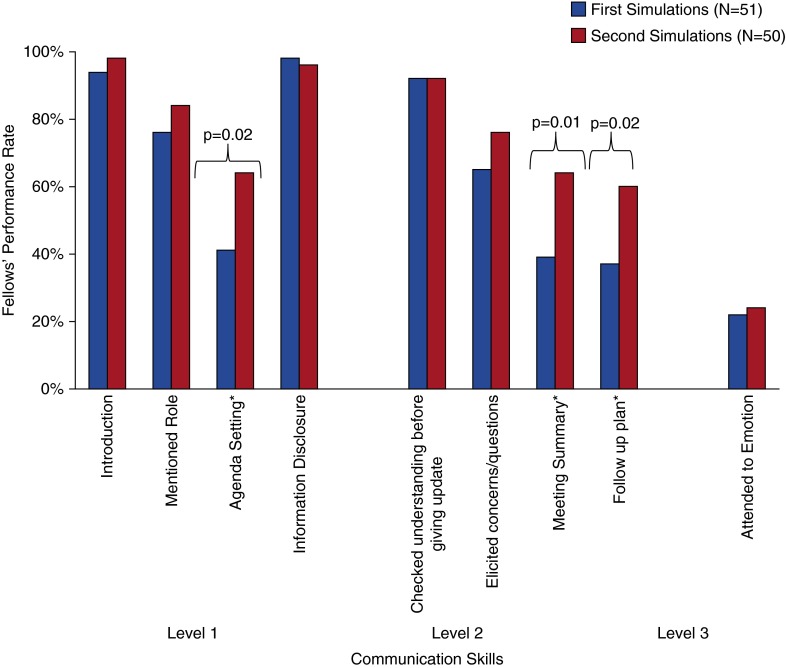
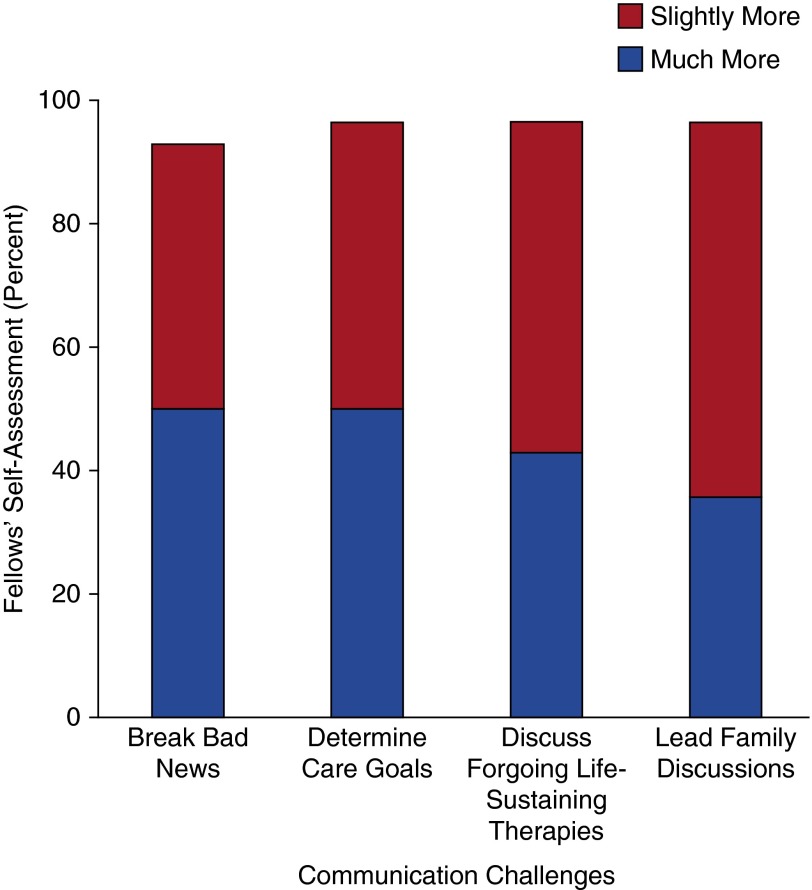
Measurements and main results: Over 3 years, 31 critical care fellows participated in the program, 28 of whom participated in 101 family meeting simulations with direct feedback by faculty facilitators. Our trainees showed high rates of information disclosure during the simulated family meetings. During the simulations done at the end of the month compared with those done at the beginning, our fellows showed significantly improved rates in: (1) verbalizing an agenda for the meeting (64 vs. 41%; Chi-square, 5.27; P = 0.02), (2) summarizing what will be done for the patient (64 vs. 39%; Chi-square, 6.21; P = 0.01), and (3) providing a follow-up plan (60 vs. 37%; Chi-square, 5.2; P = 0.02). More than 95% of our participants (n = 27) reported feeling "slightly" or "much" more comfortable with discussing foregoing life-sustaining treatment and leading family discussions after the month-long curriculum.
Conclusions: A communication skills program can be feasibly integrated into a critical care training program and is associated with improvements in fellows' skills and comfort with leading family meetings.
Keywords: communication skills; critical illness; medical education.
Figures
Comment in
-
The intensive care unit family conference. Teaching a critical intensive care unit procedure.Ann Am Thorac Soc. 2015 Apr;12(4):469-71. doi: 10.1513/AnnalsATS.201503-123ED. Ann Am Thorac Soc. 2015. PMID: 25897741 No abstract available.
References
-
- Scheunemann LP, McDevitt M, Carson SS, Hanson LC. Randomized, controlled trials of interventions to improve communication in intensive care: a systematic review. Chest. 2011;139:543–554. - PubMed
-
- Azoulay E, Chevret S, Leleu G, Pochard F, Barboteu M, Adrie C, Canoui P, Le Gall JR, Schlemmer B. Half the families of intensive care unit patients experience inadequate communication with physicians. Crit Care Med. 2000;28:3044–3049. - PubMed
-
- Curtis JR, Engelberg RA, Wenrich MD, Shannon SE, Treece PD, Rubenfeld GD. Missed opportunities during family conferences about end-of-life care in the intensive care unit. Am J Respir Crit Care Med. 2005;171:844–849. - PubMed
-
- DeVita MA, Arnold RM, Barnard D. Teaching palliative care to critical care medicine trainees. Crit Care Med. 2003;31:1257–1262. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
