

The use of inhaled prostaglandins in patients with ARDS: a systematic review and meta-analysis
- PMID: 25742022
- PMCID: PMC4451707
- DOI: 10.1378/chest.14-3161
The use of inhaled prostaglandins in patients with ARDS: a systematic review and meta-analysis
Abstract
Objective: This study aimed to determine whether inhaled prostaglandins are associated with improvement in pulmonary physiology or mortality in patients with ARDS and assess adverse effects.
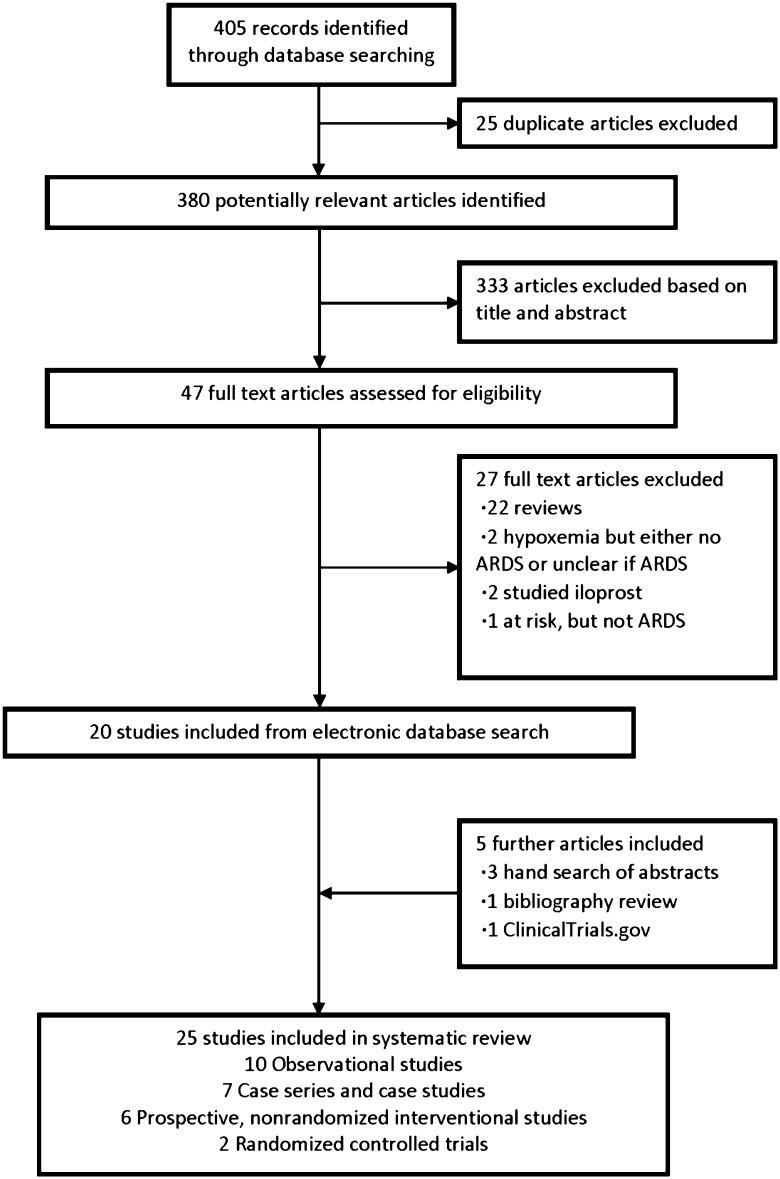
Methods: The following data sources were used: PubMed, EMBASE, CINAHL, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, reference lists, conference proceedings, and ClinicalTrials.gov. Studies selected included randomized controlled trials and nonrandomized studies. For data extraction, two reviewers independently screened titles and abstracts for eligibility. With regard to data synthesis, 25 studies (two RCTs) published over 21 years (1993-2014) were included. The PROSPERO registration number was CRD42014013180.
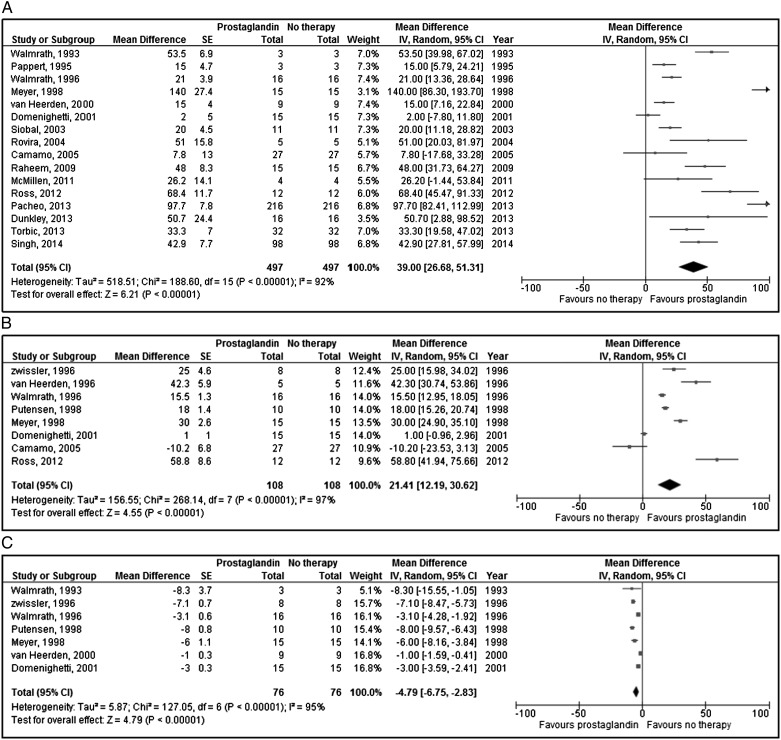
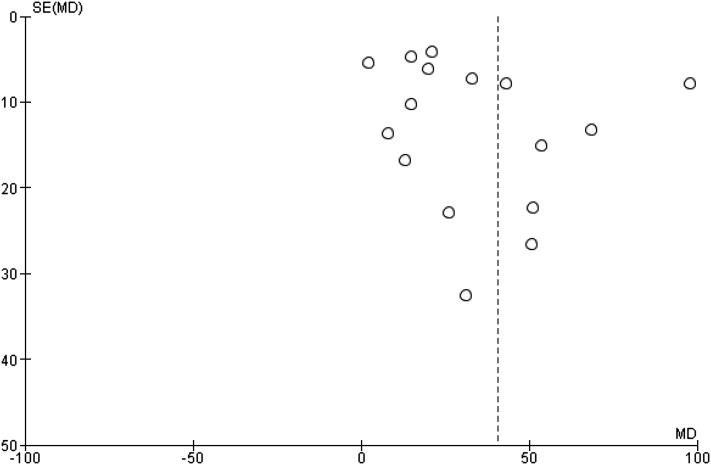
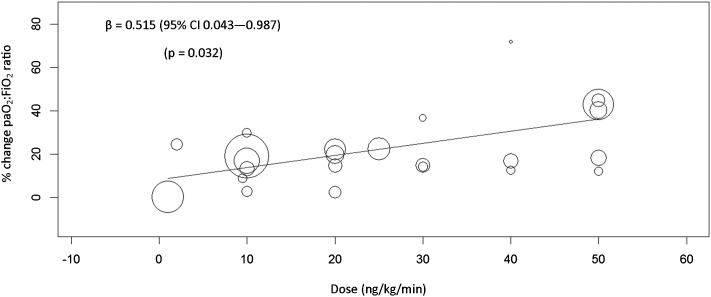
Results: One randomized controlled trial showed no difference in the change in mean Pao2 to Fio2 ratio when comparing inhaled alprostadil to placebo: 141.2 (95% CI, 120.8-161.5) to 161.5 (95% CI, 134.6-188.3) vs 163.4 (95% CI, 140.8-186.0) to 186.8 (95% CI, 162.9-210.7), P = .21. Meta-analysis of the remaining studies demonstrated that inhaled prostaglandins were associated with improvement in Pao2 to Fio2 ratio (16 studies; 39.0% higher; 95% CI, 26.7%-51.3%), and Pao2 (eight studies; 21.4% higher; 95% CI, 12.2%-30.6%), and a decrease in pulmonary artery pressure (-4.8 mm Hg; 95% CI, -6.8 mm Hg to -2.8 mm Hg). Risk of bias and heterogeneity were high. Meta-regression found no association with publication year (P = .862), baseline oxygenation (P = .106), and ARDS etiology (P = .816) with the treatment effect. Hypotension occurred in 17.4% of patients in observational studies.
Conclusions: In ARDS, inhaled prostaglandins improve oxygenation and decrease pulmonary artery pressures and may be associated with harm. Data are limited both in terms of methodologic quality and demonstration of clinical benefit. The use of inhaled prostaglandins in ARDS needs further study.
Figures
References
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute. lung injury. N Engl J Med. 2005;353(16):1685-1693. - PubMed
-
- Zapol WM, Snider MT. Pulmonary hypertension in severe acute respiratory failure. N Engl J Med. 1977;296(9):476-480. - PubMed
-
- Jardin F, Gueret P, Dubourg O, Farcot JC, Margairaz A, Bourdarias JP. Two-dimensional echocardiographic evaluation of right ventricular size and contractility in acute respiratory failure. Crit Care Med. 1985;13(11):952-956. - PubMed
-
- Squara P, Dhainaut J-F, Artigas A, Carlet J. Hemodynamic profile in severe ARDS: results of the European Collaborative ARDS Study. Intensive Care Med. 1998;24(10):1018-1028. - PubMed
-
- Sloane PJ, Gee MH, Gottlieb JE, et al. A multicenter registry of patients with acute respiratory distress syndrome. Physiology and outcome. Am Rev Respir Dis. 1992;146(2):419-426. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
