

Intraoperative functional mapping and monitoring during glioma surgery
- PMID: 25744346
- PMCID: PMC4533401
- DOI: 10.2176/nmc.ra.2014-0215
Intraoperative functional mapping and monitoring during glioma surgery
Abstract
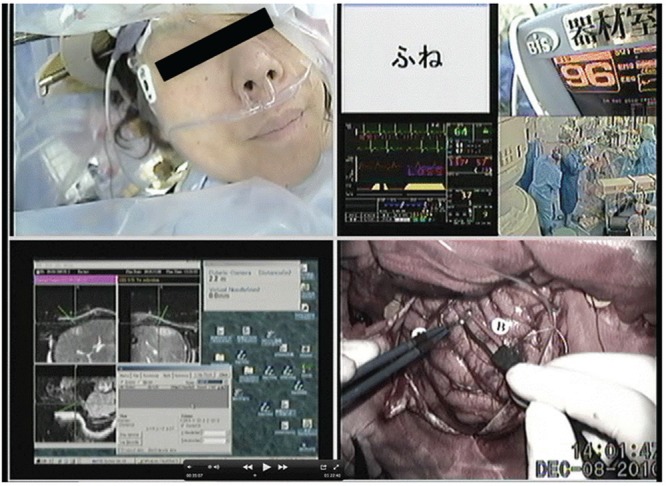
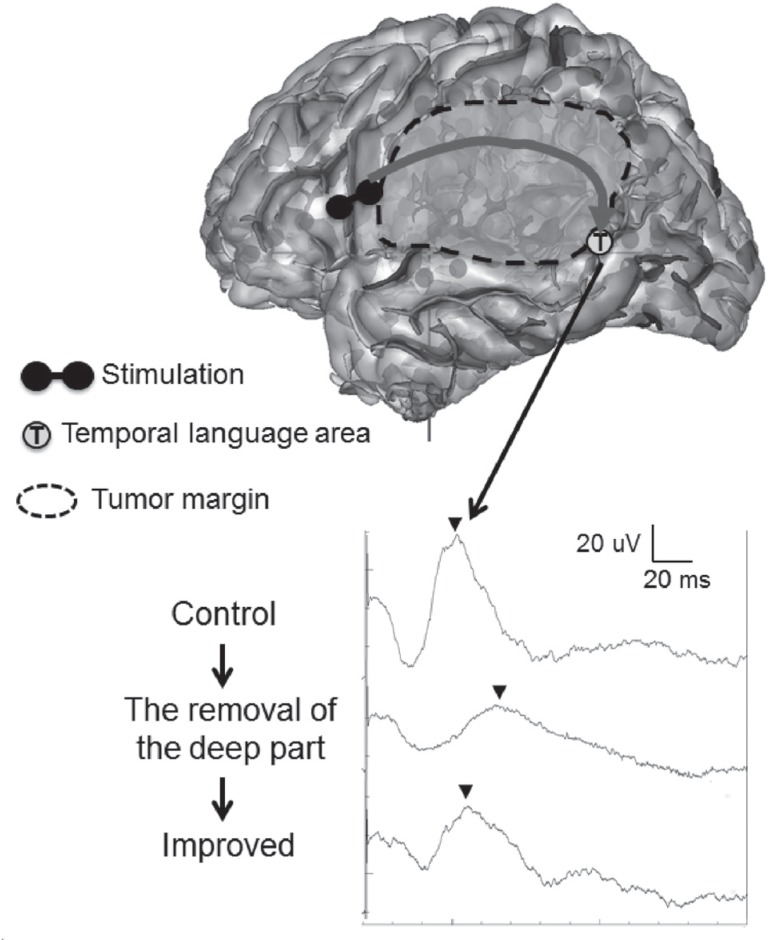
Glioma surgery represents a significant advance with respect to improving resection rates using new surgical techniques, including intraoperative functional mapping, monitoring, and imaging. Functional mapping under awake craniotomy can be used to detect individual eloquent tissues of speech and/or motor functions in order to prevent unexpected deficits and promote extensive resection. In addition, monitoring the patient's neurological findings during resection is also very useful for maximizing the removal rate and minimizing deficits by alarming that the touched area is close to eloquent regions and fibers. Assessing several types of evoked potentials, including motor evoked potentials (MEPs), sensory evoked potentials (SEPs) and visual evoked potentials (VEPs), is also helpful for performing surgical monitoring in patients under general anesthesia (GA). We herein review the utility of intraoperative mapping and monitoring the assessment of neurological findings, with a particular focus on speech and the motor function, in patients undergoing glioma surgery.
Conflict of interest statement
No conflict of interest exists. All authors who are members of The Japan Neurosurgical Society (JNS) have registered online Self-reported COI Disclosure Statement Forms through the website for JNS members.
Figures
Republished in
-
Intraoperative Functional Mapping and Monitoring during Glioma Surgery.Neurol Med Chir (Tokyo). 2015;55 Suppl 1:1-13. Neurol Med Chir (Tokyo). 2015. PMID: 26236798
References
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K, Hau P, Brandes AA, Gijtenbeek J, Marosi C, Vecht CJ, Mokhtari K, Wesseling P, Villa S, Eisenhauer E, Gorlia T, Weller M, Lacombe D, Cairncross JG, Mirimanoff RO, European Organisation for Research and Treatment of Cancer Brain Tumour and Radiation Oncology Groups; National Cancer Institute of Canada Clinical Trials Group : Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 10: 459– 466, 2009. - PubMed
-
- Sabha N, Knobbe CB, Maganti M, Al Omar S, Bernstein M, Cairns R, Cako B, von Deimling A, Capper D, Mak TW, Kiehl TR, Carvalho P, Garrett E, Perry A, Zadeh G, Guha A, Croul S: Analysis of IDH mutation, 1p/19q deletion, and PTEN loss delineates prognosis in clinical low-grade diffuse gliomas. Neuro Oncol [Epub ahead of print], 2014. - PMC - PubMed
-
- Soffietti R, Baumert BG, Bello L, von Deimling A, Duffau H, Frénay M, Grisold W, Grant R, Graus F, Hoang-Xuan K, Klein M, Melin B, Rees J, Siegal T, Smits A, Stupp R, Wick W, European Federation of Neurological Societies : Guidelines on management of low-grade gliomas: report of an EFNS-EANO Task Force. Eur J Neurol 17: 1124– 1133, 2010. - PubMed
-
- Wick W, Hartmann C, Engel C, Stoffels M, Felsberg J, Stockhammer F, Sabel MC, Koeppen S, Ketter R, Meyermann R, Rapp M, Meisner C, Kortmann RD, Pietsch T, Wiestler OD, Ernemann U, Bamberg M, Reifenberger G, von Deimling A, Weller M: NOA-04 randomized phase III trial of sequential radiochemotherapy of anaplastic glioma with procarbazine, lomustine, and vincristine or temozolomide. J Clin Oncol 27: 5874– 5880, 2009. - PubMed
-
- Lacroix M, Abi-Said D, Fourney DR, Gokaslan ZL, Shi W, DeMonte F, Lang FF, McCutcheon IE, Hassenbusch SJ, Holland E, Hess K, Michael C, Miller D, Sawaya R: A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival. J Neurosurg 95: 190– 198, 2001. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources