

Relationship of cigarette smoking with inflammation and subclinical vascular disease: the Multi-Ethnic Study of Atherosclerosis
- PMID: 25745060
- PMCID: PMC4484586
- DOI: 10.1161/ATVBAHA.114.304960
Relationship of cigarette smoking with inflammation and subclinical vascular disease: the Multi-Ethnic Study of Atherosclerosis
Abstract
Objective: We sought to assess the impact of smoking status, cumulative pack-years, and time since cessation (the latter in former smokers only) on 3 important domains of cardiovascular disease: inflammation, vascular dynamics and function, and subclinical atherosclerosis.
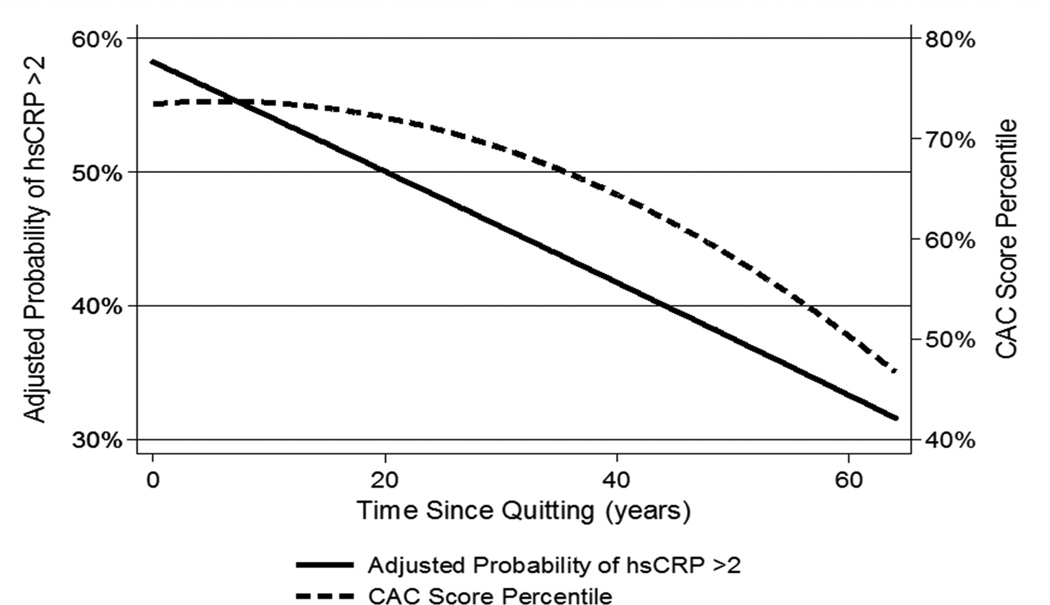
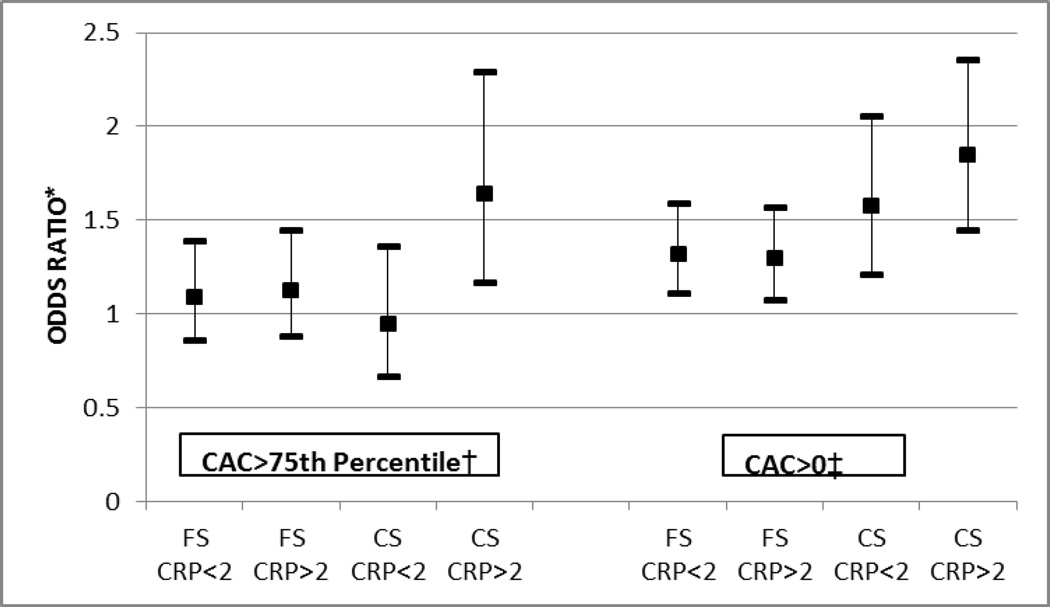
Approach and results: The Multi-Ethnic Study of Atherosclerosis (MESA) cohort enrolled 6814 adults without prior cardiovascular disease. Smoking variables were determined by self-report and confirmed with urinary cotinine. We examined cross-sectional associations between smoking parameters and (1) inflammatory biomarkers (high-sensitivity C-reactive protein [hsCRP], interleukin-6, and fibrinogen); (2) vascular dynamics and function (brachial flow-mediated dilation and carotid distensibility by ultrasound, as well as aortic distensibility by MRI); and (3) subclinical atherosclerosis (coronary artery calcification, carotid intima-media thickness, and ankle-brachial index). We identified 3218 never smokers, 2607 former smokers, and 971 current smokers. Mean age was 62 years and 47% were male. There was no consistent association between smoking and vascular distensibility or flow-mediated dilation outcomes. However, compared with never smokers, the adjusted association between current smoking and measures of either inflammation or subclinical atherosclerosis was consistently stronger than for former smoking (eg, odds ratio for hsCRP>2 mg/L of 1.7 [95% confidence interval, 1.5-2.1] versus 1.2 [1.1-1.4], odds ratio for coronary artery calcification>0 of 1.8 [1.5-2.1] versus 1.4 [1.2-1.6], respectively). Similar associations were seen for interleukin-6, fibrinogen, carotid intima-media thickness, and ankle-brachial index. A monotonic association was also found between higher pack-year quartiles and increasing inflammatory markers. Furthermore, current smokers with hsCRP>2 mg/L were more likely to have increased carotid intima-media thickness, abnormal ankle-brachial index, and coronary artery calcification>75th percentile for age, sex, and race (relative to smokers with hsCRP<2 mg/L, interaction P<0.05 for all 3 outcomes). In contrast, time since quitting in former smokers was independently associated with lower inflammation and atherosclerosis (eg, odds ratio for hsCRP>2 mg/L of 0.91 [0.88-0.95] and odds ratio for coronary artery calcification>0 of 0.94 [0.90-0.97] for every 5-year cessation interval).
Conclusions: These findings expand our understanding of the harmful effects of smoking and help explain the cardiovascular benefits of smoking cessation.
Keywords: atherosclerosis; coronary artery disease; inflammation; smoking.
© 2015 American Heart Association, Inc.
Figures
References
-
- The health consequences of smoking-50 years of progress: A report of the surgeon general. Atlanta (GA): 2014.
-
- Go AS, Mozaffarian D, Roger VL, et al. Executive summary: Heart disease and stroke statistics--2014 update: A report from the american heart association. Circulation. 2014;129:399–410. - PubMed
-
- Ambrose JA, Barua RS. The pathophysiology of cigarette smoking and cardiovascular disease: An update. Journal of the American College of Cardiology. 2004;43:1731–1737. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P50 HL120163/HL/NHLBI NIH HHS/United States
- N01-HC-95162/HC/NHLBI NIH HHS/United States
- 1 P50 HL120163-01/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01-HC-95163/HC/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- N01-HC-95165/HC/NHLBI NIH HHS/United States
- R01-HL077612/HL/NHLBI NIH HHS/United States
- N01-HC-95160/HC/NHLBI NIH HHS/United States
- N01-HC-95161/HC/NHLBI NIH HHS/United States
- N01-HC-95166/HC/NHLBI NIH HHS/United States
- N01-HC-95167/HC/NHLBI NIH HHS/United States
- N01-HC-95159/HC/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- U54 HL120163/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01-HC-95169/HC/NHLBI NIH HHS/United States
- N01-HC-95164/HC/NHLBI NIH HHS/United States
