

Frequency, cost, and risk factors of readmissions among severe sepsis survivors
- PMID: 25746745
- PMCID: PMC4479267
- DOI: 10.1097/CCM.0000000000000859
Frequency, cost, and risk factors of readmissions among severe sepsis survivors
Abstract
Objective: To determine the frequency, mortality, cost, and risk factors associated with readmission after index hospitalization with severe sepsis.
Design: Observational cohort study of Healthcare Cost and Utilization Project data.
Setting: All nonfederal hospitals in three U.S. states.
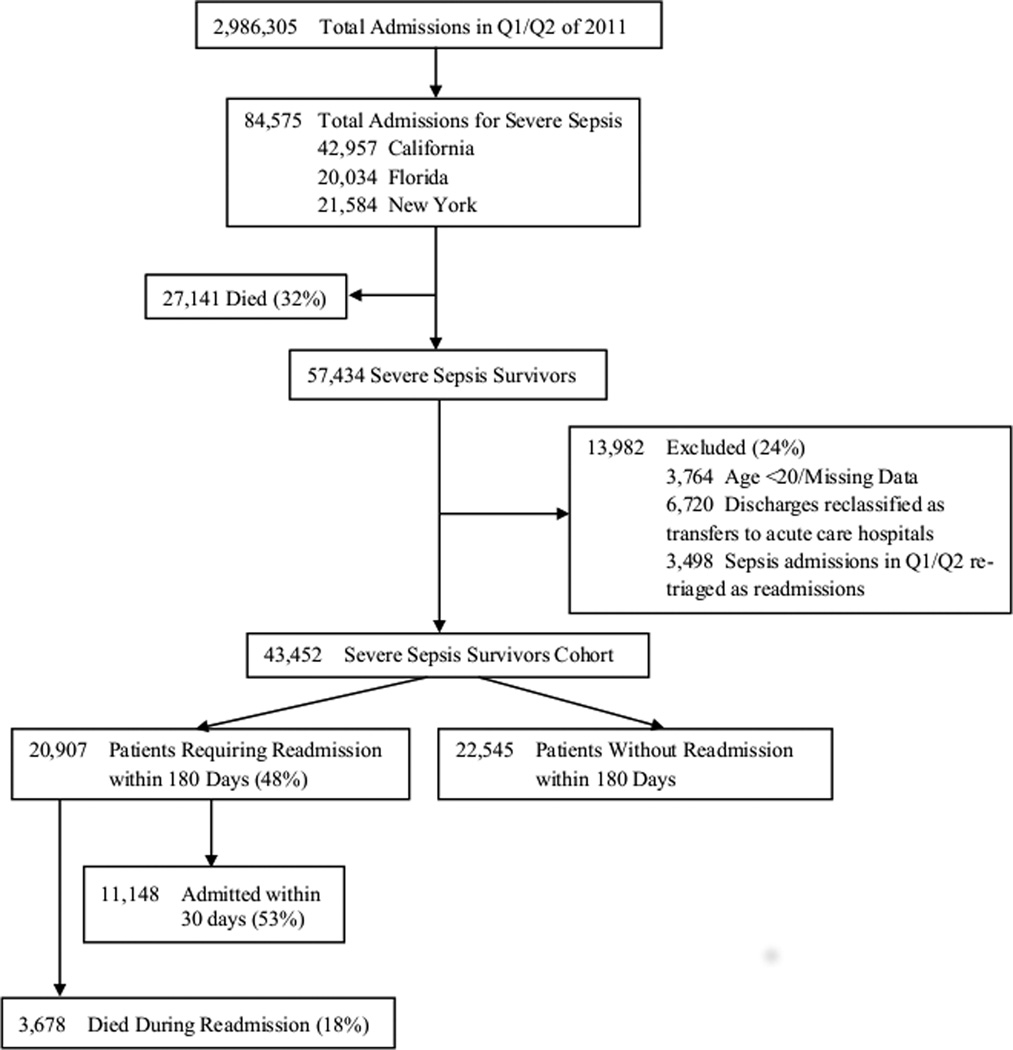
Patients: Severe sepsis survivors (n = 43,452) in the first two quarters of 2011.
Interventions: None.
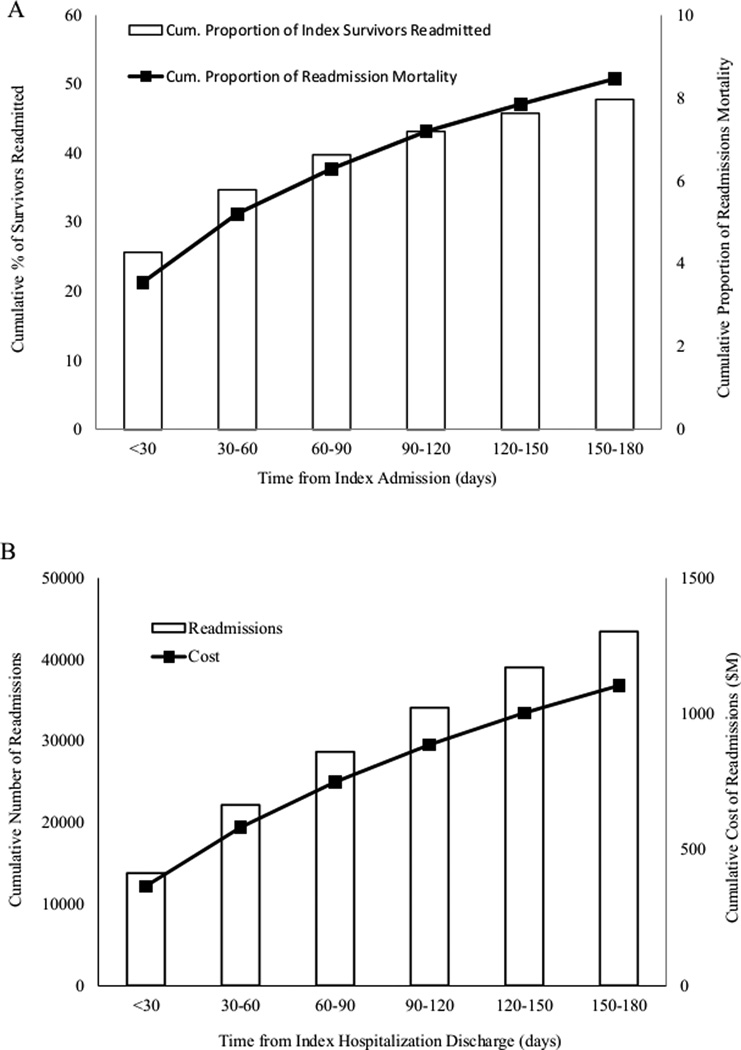
Measurements and main results: We measured readmission rates and the associated cost and mortality of readmissions in severe sepsis survivors. We used multivariable logistic regression to identify patient and hospitalization characteristics associated with readmission. Of 43,452 sepsis survivors, 26% required readmission within 30 days and 48% within 180 days. The cumulative mortality rate of sepsis survivors attributed to readmissions was 8%, and the estimated cost was over $1.1 billion. Among survivors, 25% required multiple readmissions within 180 days and accounted for 77% of all readmissions. Age younger than 80 years (odds ratio, 1.14; 95% CI, 1.08-1.21), black race (odds ratio, 1.18; 95% CI, 1.10-1.26), and Medicare or Medicaid payor status (odds ratio, 1.21; 95% CI, 1.13-1.30; odds ratio, 1.34; 95% CI, 1.23-1.46, respectively) were associated with greater odds of 30-day readmission while female gender was associated with reduced odds (odds ratio, 0.92; 95% CI, 0.87-0.96). Comorbidities including malignancy (odds ratio, 1.34; 95% CI, 1.24-1.45), collagen vascular disease (odds ratio, 1.30; 95% CI, 1.15-1.46), chronic kidney disease (odds ratio, 1.24; 95% CI, 1.18-1.31), liver disease (odds ratio, 1.22; 95% CI, 1.11-1.34), congestive heart failure (odds ratio, 1.14; 95% CI, 1.08-1.19), lung disease (odds ratio, 1.12; 95% CI, 1.06-1.18), and diabetes (odds ratio, 1.12; 95% CI, 1.07-1.17) were associated with greater odds of 30-day readmission. Index hospitalization characteristics including longer length of stay, discharge to a care facility, higher hospital annual severe sepsis case volume, and higher hospital sepsis mortality rate were also positively associated with readmission rates.
Conclusion: The 30-day and 180-day readmissions are common in sepsis survivors with significant resultant cost and mortality. Patient sociodemographics and comorbidities as well as index hospitalization characteristics are associated with 30-day readmission rates.
Conflict of interest statement
Dr. Rice disclosed that he does not have any potential conflicts of interest.
Figures
Comment in
-
How much more intelligent do we have to be about the burden of severe sepsis and septic shock?Crit Care Med. 2015 Apr;43(4):906-7. doi: 10.1097/CCM.0000000000000903. Crit Care Med. 2015. PMID: 25768351 No abstract available.
-
Sepsis Redux: Bigger and Badder Than Ever.Crit Care Med. 2015 Oct;43(10):2251-2. doi: 10.1097/CCM.0000000000001217. Crit Care Med. 2015. PMID: 26376250 No abstract available.
-
Risk Factors of Readmissions Among Severe Sepsis Survivors.Crit Care Med. 2015 Oct;43(10):e461. doi: 10.1097/CCM.0000000000001125. Crit Care Med. 2015. PMID: 26376263 No abstract available.
-
The authors reply.Crit Care Med. 2015 Oct;43(10):e461-2. doi: 10.1097/CCM.0000000000001209. Crit Care Med. 2015. PMID: 26376264 Free PMC article. No abstract available.
References
-
- MEDPAC. Report to Congress: Promoting Greater Efficiency in Medicare. 2007
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–1428. [Erratum appears in N Engl J Med. 2011 Apr 21;364(16):1582] - PubMed
-
- Ashton CM, Del Junco DJ, Souchek JP, Wray NP, Mansyur CL. The Association Between the Quality of Inpatient Care and Early Readmission: A Meta-Analysis of the Evidence. Med Care. 1997;35(10):1044–1059. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
