

Superior oblique extraocular muscle shape in superior oblique palsy
- PMID: 25747676
- PMCID: PMC4426247
- DOI: 10.1016/j.ajo.2015.02.019
Superior oblique extraocular muscle shape in superior oblique palsy
Abstract
Purpose: To investigate the superior oblique (SO) extraocular muscle cross section in normal controls and in SO palsy using high-resolution magnetic resonance imaging (MRI).
Design: Prospective observational study.
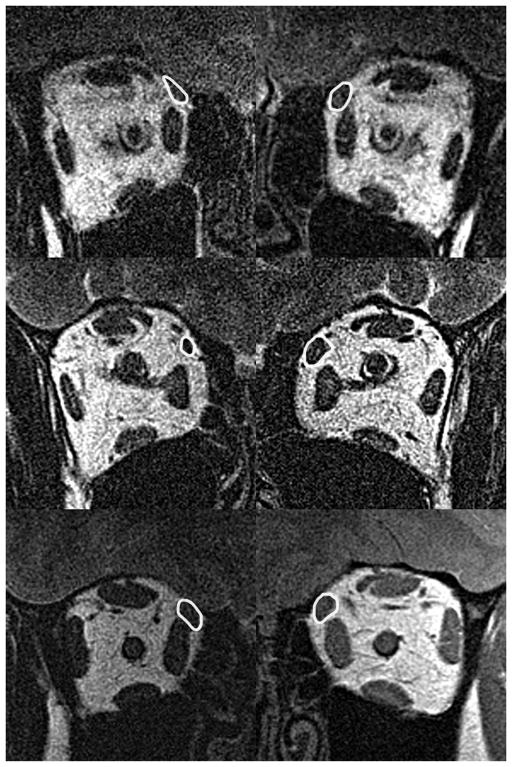
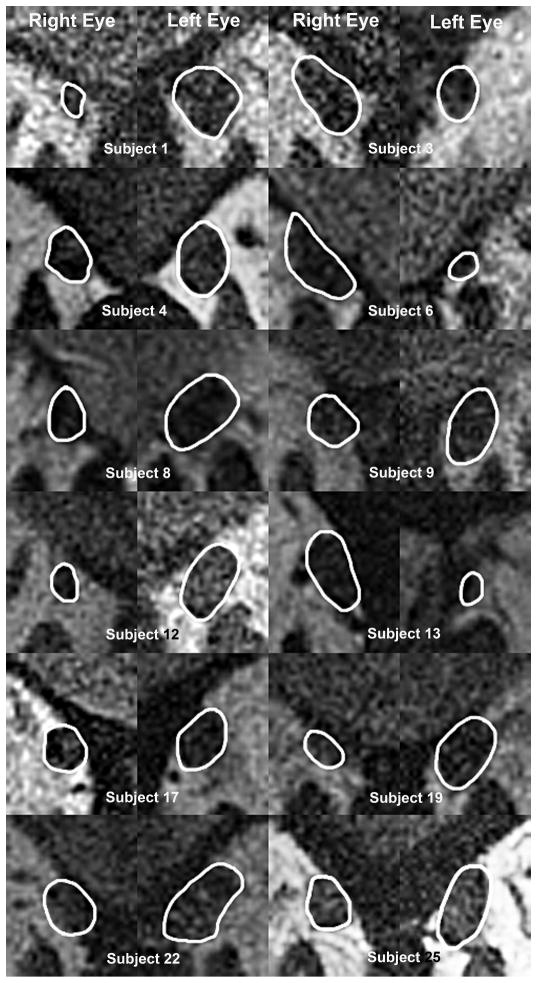
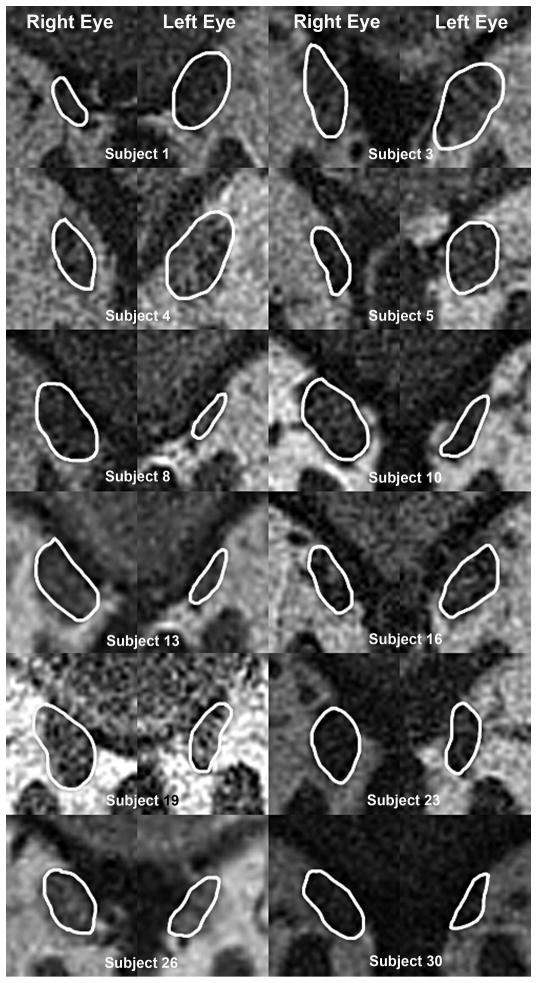
Methods: At a single academic medical center, high-resolution MRI was obtained at 312 μm in-plane resolution using surface coils in multiple, contiguous, quasi-coronal planes perpendicular to the orbital axis in 12 controls and 62 subjects with SO palsy. Previous strabismus surgery was excluded. Imaging was repeated in central gaze and infraduction. In each image plane along the SO, its cross section was outlined to compute cross-sectional area and the major and minor axes of the best-fitting ellipse. Main outcome measures were SO morphology and ocular motility.
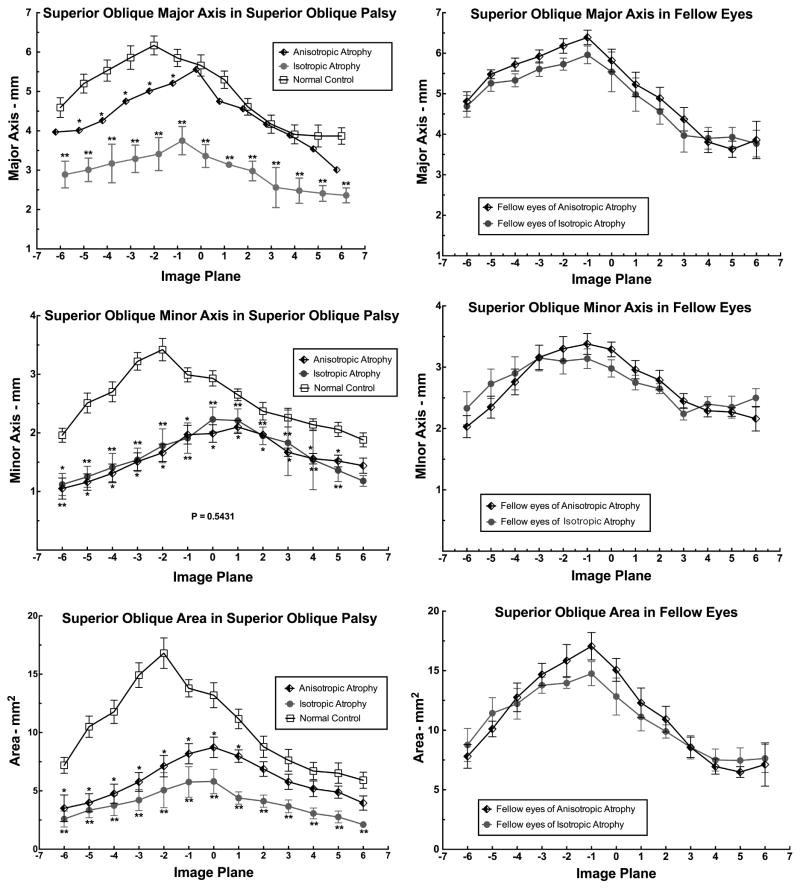
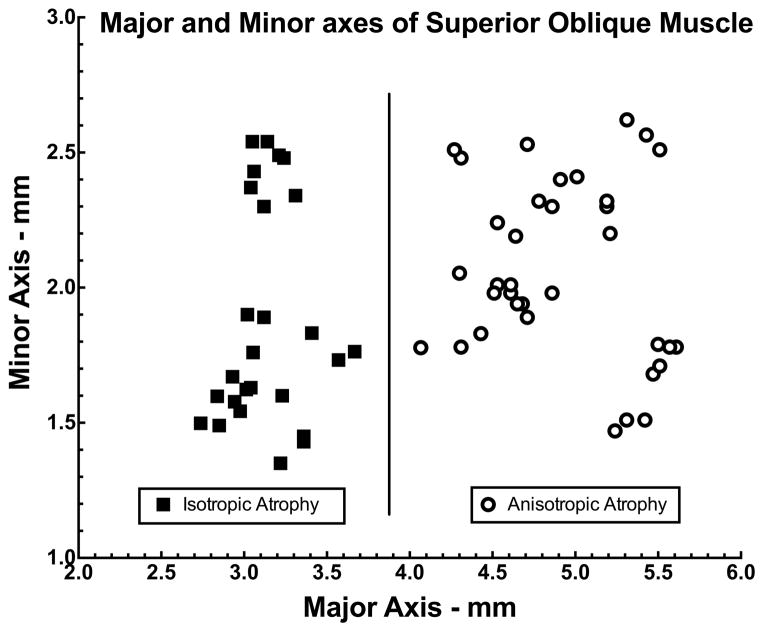
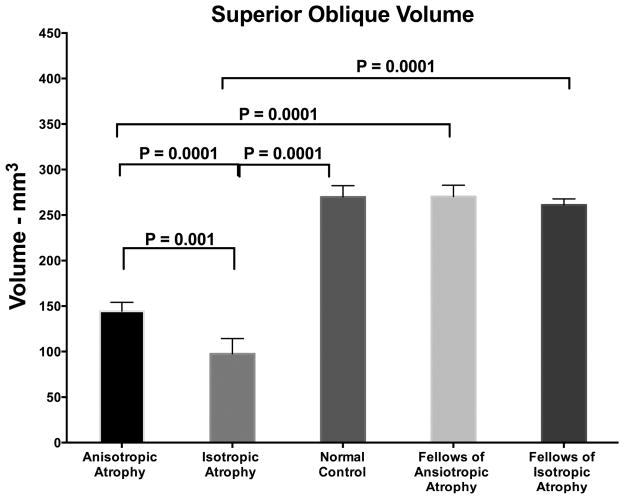
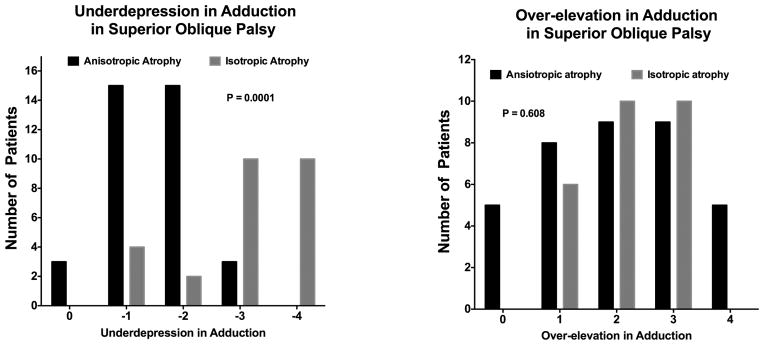
Results: The major and minor axes, cross-sectional area distributions, and volume of the SO belly were subnormal in orbits with SO palsy at most anteroposterior locations (P = .001), but discriminant analysis showed that palsied SO cross sections segregated distinctly into round and elongate shapes representing isotropic vs anisotropic atrophy, respectively. The major axis was relatively preserved in anisotropic atrophy (P = .0146). Cases with isotropic atrophy exhibited greater hypertropia in infraversion than central gaze, as well as greater excyclotorsion, than cases with anisotropic atrophy (P < .05 for all).
Conclusions: Characteristic differences in shape of the palsied SO belly correlate with different clinical features, and may reflect both the degree of differential pathology in the medial vs lateral neuromuscular SO compartments and the basis for diversity in patterns of resulting hypertropia.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Superior Oblique Extraocular Muscle Shape in Superior Oblique Palsy.Am J Ophthalmol. 2015 Oct;160(4):846-7. doi: 10.1016/j.ajo.2015.07.016. Epub 2015 Aug 4. Am J Ophthalmol. 2015. PMID: 26251124 No abstract available.
-
Reply: To PMID 25747676.Am J Ophthalmol. 2015 Oct;160(4):847. doi: 10.1016/j.ajo.2015.07.018. Epub 2015 Aug 6. Am J Ophthalmol. 2015. PMID: 26257148 No abstract available.
Similar articles
-
Magnetic resonance imaging of the functional anatomy of the inferior oblique muscle in superior oblique palsy.Ophthalmology. 2003 Jun;110(6):1219-29. doi: 10.1016/S0161-6420(03)00331-2. Ophthalmology. 2003. PMID: 12799250
-
Sensitivity of the three-step test in diagnosis of superior oblique palsy.J AAPOS. 2014 Dec;18(6):567-71. doi: 10.1016/j.jaapos.2014.08.007. Epub 2014 Nov 12. J AAPOS. 2014. PMID: 25459202 Free PMC article.
-
Rectus Pulley Displacements without Abnormal Oblique Contractility Explain Strabismus in Superior Oblique Palsy.Ophthalmology. 2016 Jun;123(6):1222-31. doi: 10.1016/j.ophtha.2016.02.016. Epub 2016 Mar 13. Ophthalmology. 2016. PMID: 26983977 Free PMC article.
-
[Diagnosis and treatment of trochlear nerve palsy].Klin Monbl Augenheilkd. 2009 Oct;226(10):806-11. doi: 10.1055/s-0028-1109680. Epub 2009 Oct 14. Klin Monbl Augenheilkd. 2009. PMID: 19830636 Review. German.
-
Recent developments in the field of superior oblique palsies.Curr Opin Ophthalmol. 2008 Sep;19(5):379-83. doi: 10.1097/ICU.0b013e328309f191. Curr Opin Ophthalmol. 2008. PMID: 18772669 Review.
Cited by
-
Isolated schwannoma involving extraocular muscles.J AAPOS. 2016 Aug;20(4):343-7. doi: 10.1016/j.jaapos.2016.05.015. Epub 2016 Jul 14. J AAPOS. 2016. PMID: 27424045 Free PMC article.
-
Masquerading Superior Oblique Palsy.Am J Ophthalmol. 2022 Oct;242:197-208. doi: 10.1016/j.ajo.2022.05.017. Epub 2022 May 23. Am J Ophthalmol. 2022. PMID: 35618024 Free PMC article.
-
Predictive factors for corrective effect of inferior rectus recession for congenital superior oblique palsy.Graefes Arch Clin Exp Ophthalmol. 2018 Feb;256(2):403-409. doi: 10.1007/s00417-017-3838-z. Epub 2017 Nov 7. Graefes Arch Clin Exp Ophthalmol. 2018. PMID: 29116398
-
Extraocular Muscle Compartments in Superior Oblique Palsy.Invest Ophthalmol Vis Sci. 2016 Oct 1;57(13):5535-5540. doi: 10.1167/iovs.16-20172. Invest Ophthalmol Vis Sci. 2016. PMID: 27768791 Free PMC article.
-
Functional morphometry demonstrates extraocular muscle compartmental contraction during vertical gaze changes.J Neurophysiol. 2016 Jan 1;115(1):370-8. doi: 10.1152/jn.00825.2015. Epub 2015 Nov 4. J Neurophysiol. 2016. PMID: 26538608 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
