

Insulin resistance, metabolic syndrome, and lung function in US adolescents with and without asthma
- PMID: 25748066
- PMCID: PMC4530022
- DOI: 10.1016/j.jaci.2015.01.010
Insulin resistance, metabolic syndrome, and lung function in US adolescents with and without asthma
Abstract
Background: Obesity increases both the risk of asthma and asthma severity and is a well-known risk factor for insulin resistance and the metabolic syndrome (MS) in children and adolescents.
Objective: We aimed to examine the association among obesity, insulin sensitivity, MS, and lung function in US adolescents with and without asthma.
Methods: We performed a cross-sectional study of 1429 adolescents aged 12 to 17 years in the 2007-2010 National Health and Nutrition Examination Survey. Adjusted regression was used to assess the relationships among obesity, insulin sensitivity/resistance, MS, and lung function in children with and without asthma.
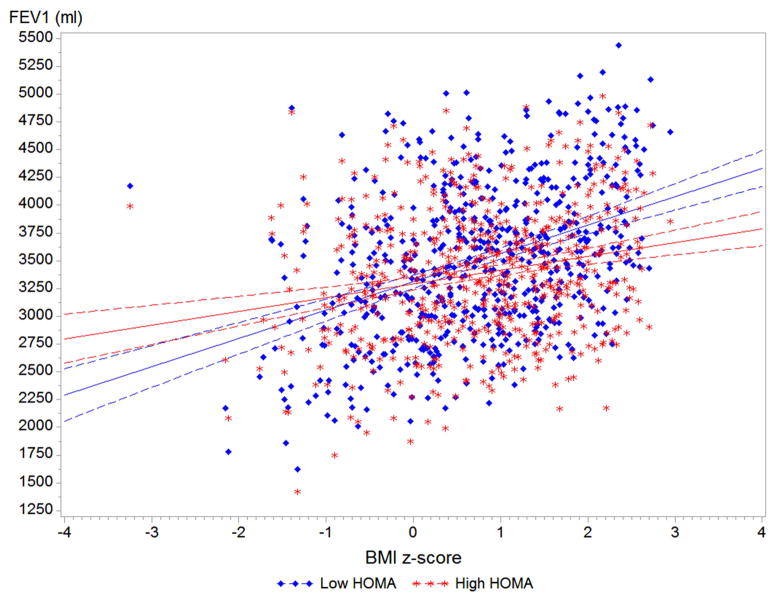
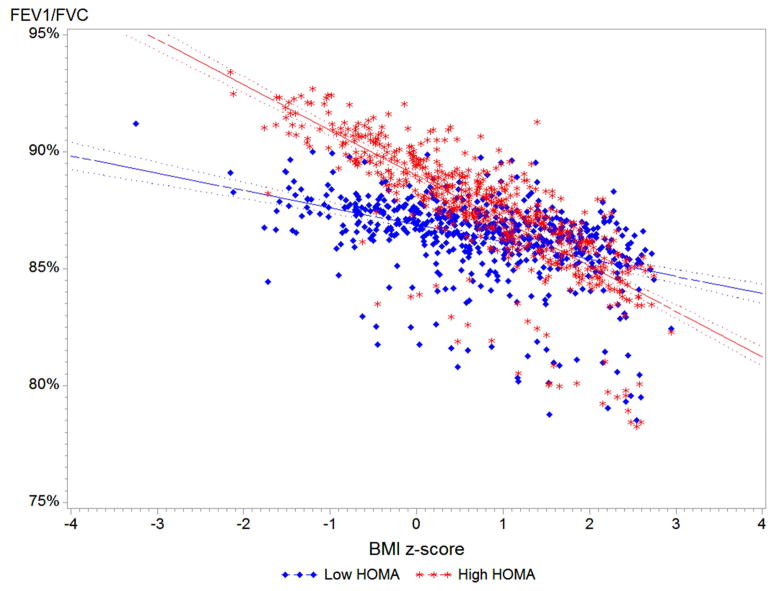
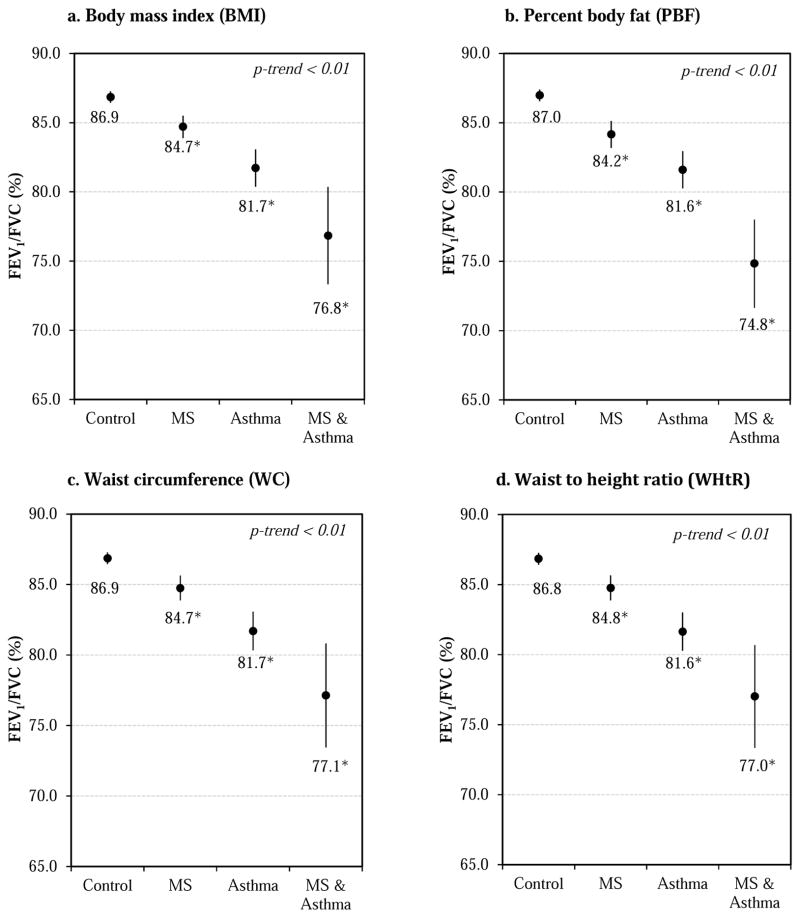
Results: Insulin resistance was negatively associated with FEV1 and forced vital capacity (FVC) in adolescents with and without asthma, whereas MS was associated with lower FEV1/FVC ratios, with a more pronounced decrease found among asthmatic patients; these associations were driven by overweight/obese adolescents. Higher body mass index was associated with a decrease in FEV1/FVC ratios among adolescents with insulin resistance. Compared with healthy participants, adolescents with MS had an approximately 2% decrease in FEV1/FVC ratios, adolescents with asthma had an approximately 6% decrease, and those with MS and asthma had approximately 10% decreased FEV1/FVC ratios (P < .05).
Conclusion: Insulin resistance and MS are associated with worsened lung function in overweight/obese adolescents. Asthma and MS synergistically decrease lung function, as do obesity and insulin resistance. These factors might contribute to the pathogenesis of asthma severity in obese patients and warrant further investigation.
Keywords: Asthma; National Health and Nutrition Examination Survey; adiposity; insulin resistance; lung function; metabolic syndrome; obesity.
Copyright © 2015 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Plasminogen activator inhibitor-1, fibrinogen, and lung function in adolescents with asthma and obesity.Endocr Res. 2012;37(3):135-44. doi: 10.3109/07435800.2012.654555. Epub 2012 May 11. Endocr Res. 2012. PMID: 22578058
-
Insulin resistance and lung function in obese asthmatic pre-pubertal children.J Pediatr Endocrinol Metab. 2018 Jan 26;31(1):45-51. doi: 10.1515/jpem-2017-0182. J Pediatr Endocrinol Metab. 2018. PMID: 29332017 Clinical Trial.
-
Association of pulmonary function with adiposity and metabolic abnormalities in urban minority adolescents.Ann Am Thorac Soc. 2014 Jun;11(5):744-52. doi: 10.1513/AnnalsATS.201311-403OC. Ann Am Thorac Soc. 2014. PMID: 24785169 Free PMC article.
-
Metabolic risk-factor clustering estimation in children: to draw a line across pediatric metabolic syndrome.Int J Obes (Lond). 2007 Apr;31(4):591-600. doi: 10.1038/sj.ijo.0803581. Int J Obes (Lond). 2007. PMID: 17384660 Review.
-
Metabolic syndrome in young people.Curr Opin Endocrinol Diabetes Obes. 2014 Feb;21(1):56-63. doi: 10.1097/01.med.0000436414.90240.2c. Curr Opin Endocrinol Diabetes Obes. 2014. PMID: 24247648 Review.
Cited by
-
Not Only Metabolic Complications of Childhood Obesity.Nutrients. 2024 Feb 15;16(4):539. doi: 10.3390/nu16040539. Nutrients. 2024. PMID: 38398863 Free PMC article. Review.
-
Humoral immune factors and asthma among American Indian children: a case-control study.BMC Pulm Med. 2016 Jun 13;16(1):93. doi: 10.1186/s12890-016-0257-6. BMC Pulm Med. 2016. PMID: 27295946 Free PMC article.
-
SARS-CoV-2 infection impairs the insulin/IGF signaling pathway in the lung, liver, adipose tissue, and pancreatic cells via IRF1.Metabolism. 2022 Aug;133:155236. doi: 10.1016/j.metabol.2022.155236. Epub 2022 Jun 8. Metabolism. 2022. PMID: 35688210 Free PMC article.
-
Caloric restriction prevents the development of airway hyperresponsiveness in mice on a high fat diet.Sci Rep. 2019 Jan 22;9(1):279. doi: 10.1038/s41598-018-36651-2. Sci Rep. 2019. PMID: 30670753 Free PMC article.
-
Impact of Evolutionary Changes in Nonalcoholic Fatty Liver Disease on Lung Function Decline.Gut Liver. 2023 Jan 15;17(1):139-149. doi: 10.5009/gnl210545. Epub 2022 May 25. Gut Liver. 2023. PMID: 35611668 Free PMC article.
References
-
- Akinbami LJ, Moorman JE, Bailey C, Zahran HS, King M, Johnson CA, Liu X. Trends in asthma prevalence, health care use, and mortality in the united states, 2001–2010. NCHS data brief. 2012:1–8. - PubMed
-
- Akinbami LJ, Moorman JE, Garbe PL, Sondik EJ. Status of childhood asthma in the united states, 1980–2007. Pediatrics. 2009;123 (Suppl 3):S131–145. - PubMed
-
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity among adults: United states, 2011–2012. NCHS data brief. 2013:1–8. - PubMed
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the united states, 1999–2004. JAMA: the journal of the American Medical Association. 2006;295:1549–1555. - PubMed
-
- Dixon AE, Holguin F, Sood A, Salome CM, Pratley RE, Beuther DA, Celedon JC, Shore SA, Lung D American Thoracic Society Ad Hoc Subcommittee on O. An official american thoracic society workshop report: Obesity and asthma. Proc Am Thorac Soc. 2010;7:325–335. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
