

Effect of provider prompts on adolescent immunization rates: a randomized trial
- PMID: 25748976
- PMCID: PMC8340134
- DOI: 10.1016/j.acap.2014.10.006
Effect of provider prompts on adolescent immunization rates: a randomized trial
Abstract
Objective: Adolescent immunization rates are suboptimal. Experts recommend provider prompts at health care visits to improve rates. We assessed the impact of either electronic health record (EHR) or nurse- or staff-initiated provider prompts on adolescent immunization rates.
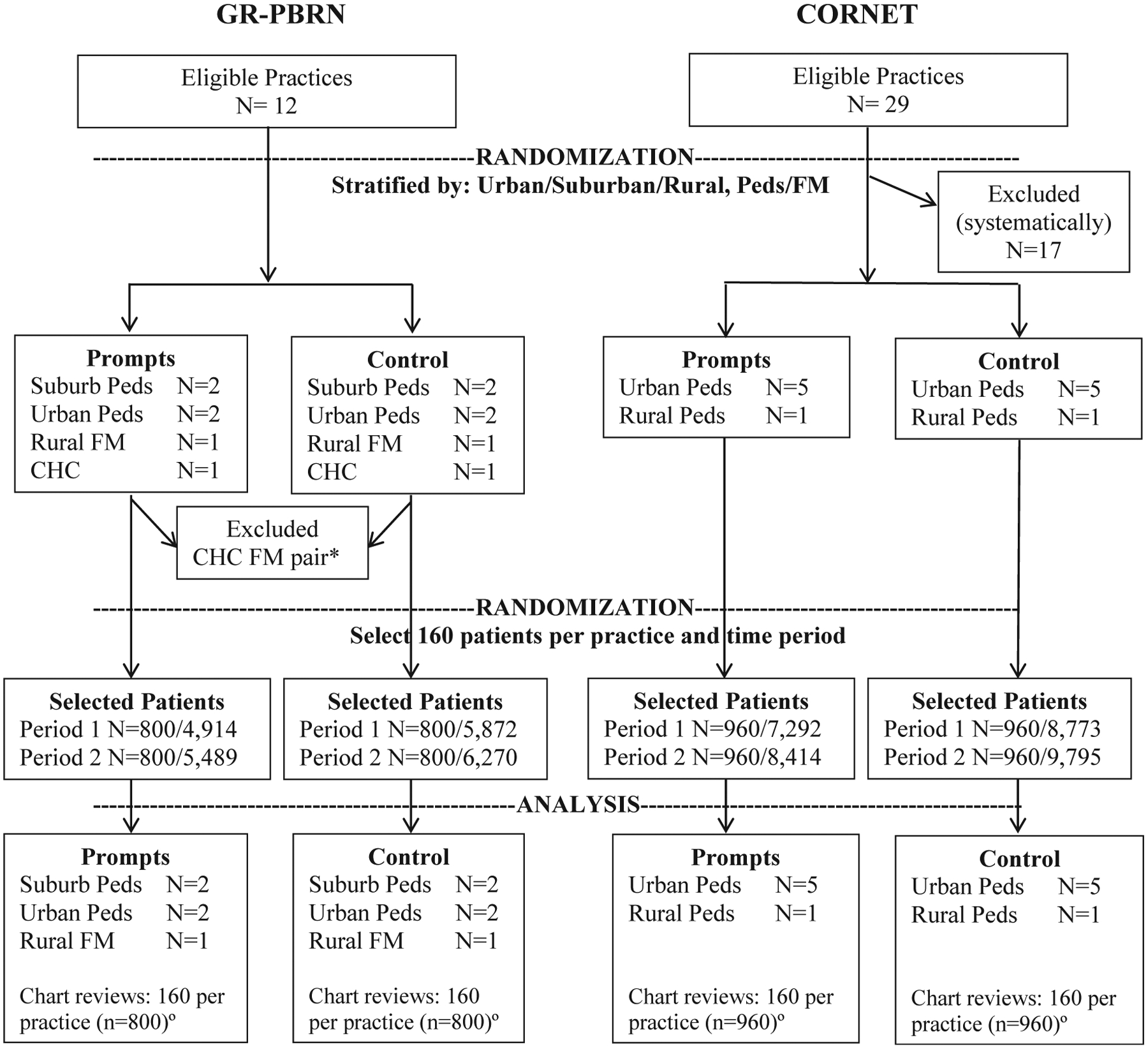
Methods: We conducted a randomized controlled trial, allocating practices in 1 of 2 practice-based research networks (PBRN) to provider prompts or standard-of-care control. Ten primary care practices participated, 5 intervention and 5 controls, each matched in pairs on urban, suburban, or rural location and practice type (pediatric or family medicine), from a PBRN in Greater Rochester, New York (GR-PBRN); and 12 practices, 6 intervention, 6 controls, similarly matched, from a national pediatric continuity clinic PBRN (CORNET). The study period was 1 year per practice, ranging from June 2011 to January 2013. Study participants were adolescents 11 to 17 years attending these 22 practices; random sample of chart reviews per practice for baseline and postintervention year to assess immunization rates (n = 7,040 total chart reviews for adolescents with >1 visit in a period). The intervention was an EHR prompt (4 GR-PBRN and 5 CORNET practice pairs) (alert) that appeared on providers' computer screens at all office visits, indicating the specific immunizations that adolescents were recommended to receive. Staff prompts (1 GR-PBRN pair and 1 CORNET pair) in the form of a reminder sheet was placed on the provider's desk in the exam room indicating the vaccines due. We compared immunization rates, stratified by PBRN, for routine vaccines (meningococcus, pertussis, human papillomavirus, influenza) at study beginning and end.
Results: Intervention and control practices within each PBRN were similar at baseline for demographics and immunization rates. Immunization rates at the study end for adolescents who were behind on immunizations at study initiation were not significantly different for intervention versus control practices for any vaccine or combination of vaccines. Results were similar for each PBRN and also when only EHR-based prompts was assessed. For example, at study end, 3-dose human papillomavirus vaccination rates for GR-PBRN intervention versus control practices were 51% versus 53% (adjusted odds ratio 0.96; 95% confidence interval 0.64-1.34); CORNET intervention versus control rates were 50% versus 42% (adjusted odds ratio 1.06; 95% confidence interval 0.68-1.88).
Conclusions and relevance: In both a local and national setting, provider prompts failed to improve adolescent immunization rates. More rigorous practice-based changes are needed.
Keywords: EHR; HPV; Tdap; adolescent immunization; influenza; meningococcal; outreach; provider prompt.
Copyright © 2015. Published by Elsevier Inc.
Conflict of interest statement
The other authors declare that they have no conflict of interest.
Figures
References
-
- Fiore AE, Uyeki TM, Broder K, et al. Prevention and control of influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Recomm Rep. 2010;59(RR-8):1–62. - PubMed
-
- US Centers for Disease Control and Prevention. National and state vaccination coverage among adolescents aged 13–17 years—United States, 2011. MMWR Morb Mortal Wkly Rep. 2012;61:671–677. - PubMed
-
- US Centers for Disease Control and Prevention. Flu vaccination coverage, United States, 2012–13 influenza season. Available at: http://www.cdc.gov/flu/fluvaxview/coverage-1213estimates.htm. Accessed January 23, 2015.
-
- US Centers for Disease Control and Prevention. National and state vaccination coverage among adolescents aged 13 through 17 years—United States, 2010. MMWR Morb Mortal Wkly Rep. 2011;60:1117–1123. - PubMed
