

Monomelic amyotrophy (hirayama disease) with upper motor neuron signs: a case report
- PMID: 25750881
- PMCID: PMC4351483
- DOI: 10.5535/arm.2015.39.1.122
Monomelic amyotrophy (hirayama disease) with upper motor neuron signs: a case report
Abstract
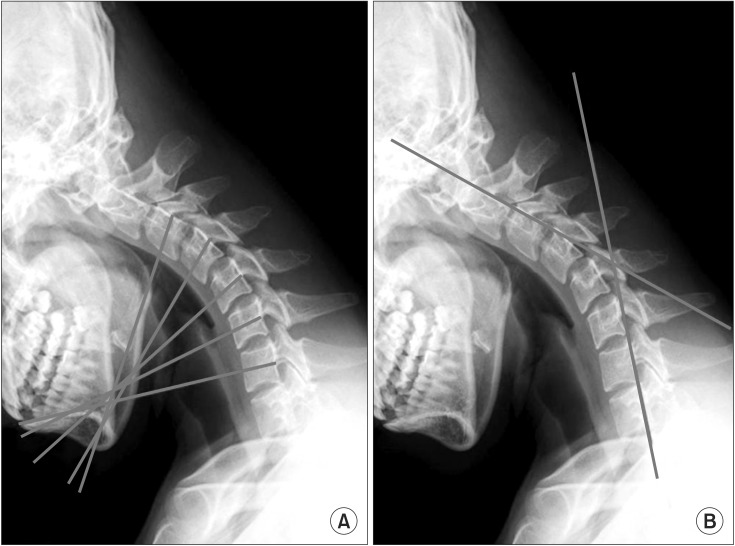
Monomelic amyotrophy (MMA), also known as Hirayama disease, is a sporadic juvenile muscular atrophy in the distal upper extremities. This disorder rarely involves proximal upper extremities and presents minimal sensory symptoms with no upper motor neuron (UMN) signs. It is caused by anterior displacement of the posterior dural sac and compression of the cervical cord during neck flexion. An 18-year-old boy visited our clinic with a 5-year history of left upper extremity pain and slowly progressive weakness affecting the left shoulder. Atrophy was present in the left supraspinatus and infraspinatus. On neurological examination, positive UMN signs were evident in both upper and lower extremities. Electrodiagnostic study showed root lesion involving the fifth to seventh cervical segment of the cord with chronic and ongoing denervation in the fifth and sixth cervical segment innervated muscles. Cervical magnetic resonance imaging (MRI) showed asymmetric cord atrophy apparent in the left side and intramedullary high signal intensity along the fourth to sixth cervical vertebral levels. With neck flexion, cervical MRI revealed anterior displacement of posterior dural sac, which results in the cord compression of those segments. The mechanisms of myelopathy in our patient seem to be same as that of MMA. We report a MMA patient involving proximal limb with UMN signs in biomechanical concerns and discuss clinical importance of cervical MRI with neck flexion. The case highlights that clinical variation might cause misdiagnosis.
Keywords: Biological assays; Monomelic amyotrophy; Pyramidal signs.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures


References
-
- Xu X, Han H, Gao H, Hou C, Fan D, Fu Y, et al. The increased range of cervical flexed motion detected by radiographs in Hirayama disease. Eur J Radiol. 2011;78:82–86. - PubMed
-
- Tashiro K, Kikuchi S, Itoyama Y, Tokumaru Y, Sobue G, Mukai E, et al. Nationwide survey of juvenile muscular atrophy of distal upper extremity (Hirayama disease) in Japan. Amyotroph Lateral Scler. 2006;7:38–45. - PubMed
-
- Pradhan S. Bilaterally symmetric form of Hirayama disease. Neurology. 2009;72:2083–2089. - PubMed
-
- Yilmaz O, Alemdaroglu I, Karaduman A, Haliloglu G, Topaloglu H. Benign monomelic amyotrophy in a 7-year-old girl with proximal upper limb involvement: case report. Turk J Pediatr. 2011;53:471–476. - PubMed
-
- Kato Y, Kataoka H, Ichihara K, Imajo Y, Kojima T, Kawano S, et al. Biomechanical study of cervical flexion myelopathy using a three-dimensional finite element method. J Neurosurg Spine. 2008;8:436–441. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
