

Prevalence and correlation of infectious agents in hospitalized children with acute respiratory tract infections in Central China
- PMID: 25751402
- PMCID: PMC4353725
- DOI: 10.1371/journal.pone.0119170
Prevalence and correlation of infectious agents in hospitalized children with acute respiratory tract infections in Central China
Abstract
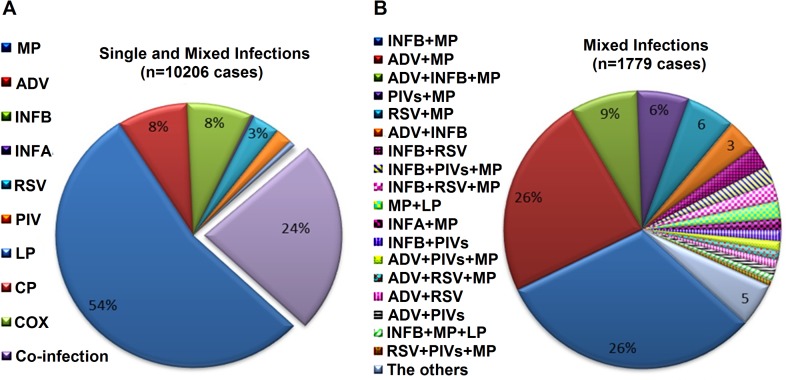
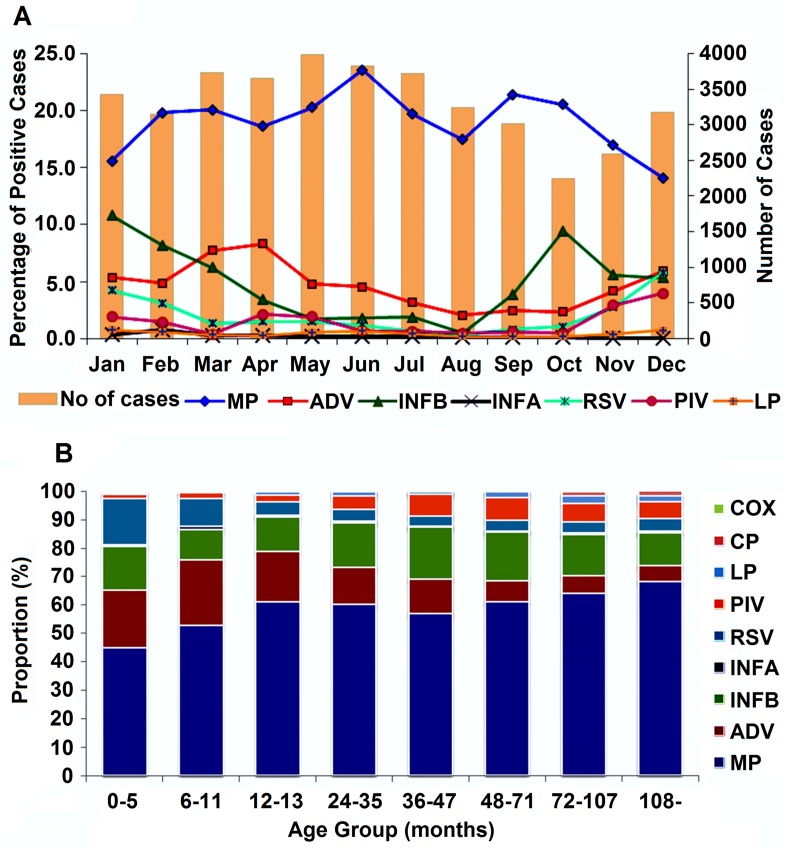
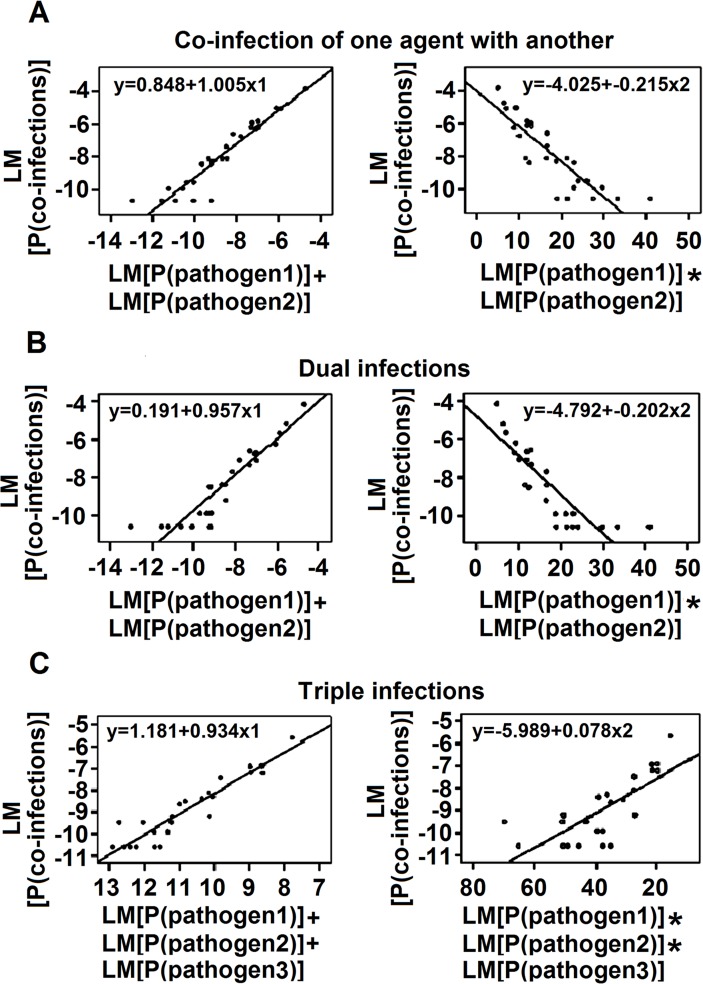
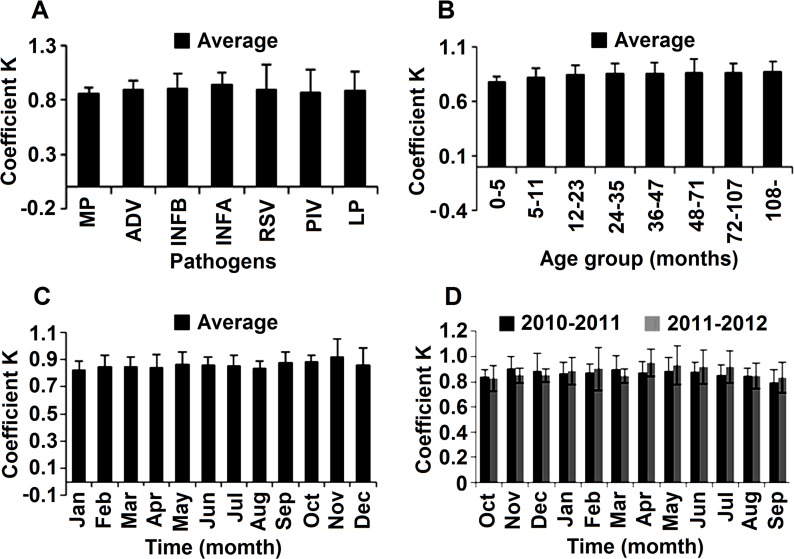
Acute respiratory tract infections (ARTIs) are associated with significant morbidity and mortality worldwide, especially in children under the age of 5 years. Almost 2 million children die from ARTIs each year, and most of them are from developing countries. The prevalence and correlation of pathogens in ARTIs are poorly understood, but are critical for improving case prevention, treatment, and management. In this study, we investigated the prevalence and correlation of infectious agents in children with ARTIs. A total of 39,756 children with one or more symptoms, including fever, cough, sore throat, tonsillitis, pharyngitis, herpangina, pneumonia, and bronchiolitis, were enrolled in the study. All patients were hospitalized in Wuhan Children's Hospital between October 1, 2010 and September 30, 2012, and were evaluated for infectious agents. Pathogens, including Mycoplasma pneumoniae, influenza A virus, influenza B virus, adenoviruses, respiratory syncytial virus, parainfluenza virus, Legionella pneumophila, Chlamydophila pneumoniae, and Coxiella burnetii, were screened simultaneously in patient blood samples using anti-pathogen IgM tests. Regression analysis was used to reveal correlations among the pathogens. Our results showed that one or more pathogens were identified in 10,206 patients, and that Mycoplasma pneumoniae, adenoviruses, and influenza B virus were the leading infectious agents. Mixed-infections of pathogens were detected in 2,391 cases, with Mycoplasma pneumoniae as the most frequent pathogen. The most common agents in the co-infections were Mycoplasma pneumoniae and influenza B virus. Regression analysis revealed a linear correlation between the proportion of mixed infections and the incidence of multi-pathogen infections. The prevalence of infectious agents in children with ARTIs was determined. Equations were established to estimate multiple infections by single-pathogen detection. This revealed a linear correlation for pathogens in children with ARTIs. This study provides useful information for improving case prevention and management.
Conflict of interest statement
Figures
References
-
- Williams BG, Gouws E, Boschi-Pinto C, Bryce J, Dye C. Estimates of world-wide distribution of child deaths from acute respiratory infections. Lancet Infect Dis. 2002;2: 25–32. - PubMed
-
- McIntosh K. Community-acquired pneumonia in children. N Engl J Med. 2002;346: 429–437. - PubMed
-
- Dwigh A, Powell A. Mycoplasmal infection. In Nellson’ Textbook of Pediatrics, 1996; Vol, Chapter 196:824–827.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
