

Lateral Ventricle Volume Asymmetry Predicts Midline Shift in Severe Traumatic Brain Injury
- PMID: 25752227
- PMCID: PMC4545563
- DOI: 10.1089/neu.2014.3696
Lateral Ventricle Volume Asymmetry Predicts Midline Shift in Severe Traumatic Brain Injury
Abstract
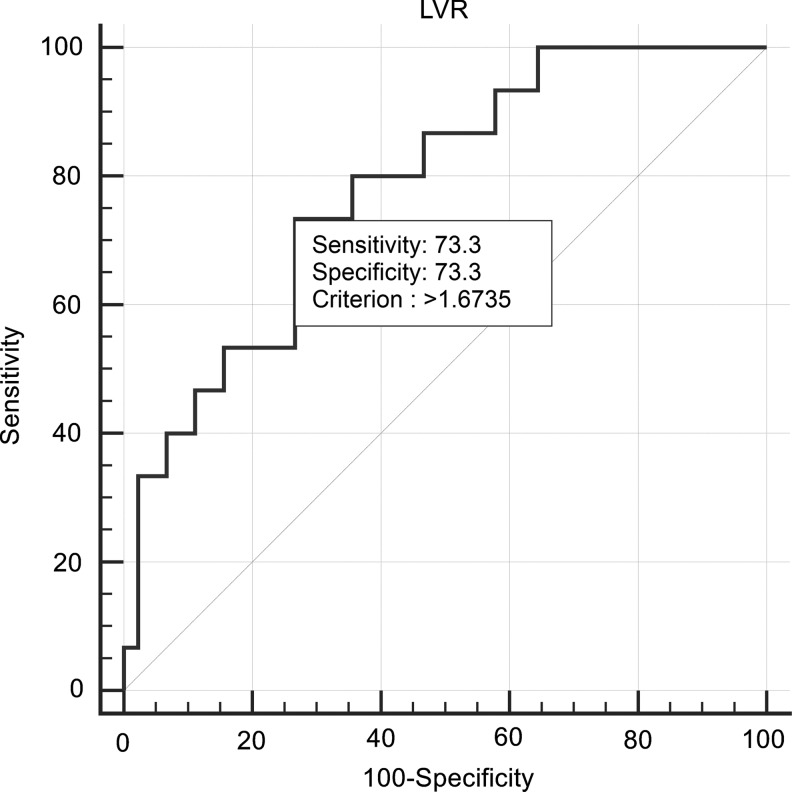
Midline shift following severe traumatic brain injury (sTBI) detected on computed tomography (CT) scans is an established predictor of poor outcome. We hypothesized that lateral ventricular volume (LVV) asymmetry is an earlier sign of developing asymmetric intracranial pathology than midline shift. This retrospective analysis was performed on data from 84 adults with blunt sTBI requiring a ventriculostomy who presented to a Level I trauma center. Seventy-six patients underwent serial CTs within 3 h and an average of three scans within the first 10 d of sTBI. Left and right LVVs were quantified by computer-assisted manual volumetric measurements. LVV ratios (LVR) were determined on the admission CT to evaluate ventricular asymmetry. The relationship between the admission LVR value and subsequent midline shift development was tested using receiver operating characteristic (ROC) analysis, and odds ratio (OR) and relative risk tests. Sixty patients had no >5 mm midline shift on the initial admission scan. Of these, 15 patients developed it subsequently (16 patients already had >5 mm midline shift on admission scans). For >5 mm midline shift development, admission LVR of >1.67 was shown to have a sensitivity of 73.3% and a specificity of 73.3% (area under the curve=0.782; p<0.0001). LVR of >1.67 as exposure yielded an OR of 7.56 (p<0.01), and a risk ratio of 4.42 (p<0.01) for midline shift development as unfavorable outcome. We propose that LVR captures LVV asymmetry and is not only related to, but also predicts the development of midline shift already at admission CT examination. Lateral ventricles may have a higher "compliance" than midline structures to developing asymmetric brain pathology. LVR analysis is simple, rapidly accomplished and may allow earlier interventions to attenuate midline shift and potentially improve ultimate outcomes.
Keywords: computed tomography; midline shift; traumatic brain injury; ventricle.
Figures



References
-
- Bruns J., Jr., and Hauser W.A. (2003). The epidemiology of traumatic brain injury: a review. Epilepsia 44 Suppl 10, 2–10 - PubMed
-
- Cole T.B. (2004). Global road safety crisis remedy sought: 1.2 million killed, 50 million injured annually. JAMA 291, 2531–2532 - PubMed
-
- Andriessen T.M., Horn J., Franschman G., van der Naalt J., Haitsma I., Jacobs B., Steyerberg E.W., and Vos P.E. (2011). Epidemiology, severity classification, and outcome of moderate and severe traumatic brain injury: a prospective multicenter study. J. Neurotrauma 28, 2019–2031 - PubMed
-
- Zee C.S. and Go J.L. (1998). CT of head trauma. Neuroimaging Clin. N. Am. 8, 525–539 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
