

Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study
- PMID: 25752327
- PMCID: PMC4691343
- DOI: 10.1111/liv.12818
Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study
Abstract
Background & aims: Hepatocellular carcinoma (HCC) is the second most common cause of cancer deaths worldwide. The global HCC BRIDGE study was a multiregional, large-scale, longitudinal cohort study undertaken to improve understanding of real-life management of patients with HCC, from diagnosis to death.
Methods: Data were collected retrospectively from January 2005 to September 2012 by chart reviews of eligible patients newly diagnosed with HCC at participating institutions.
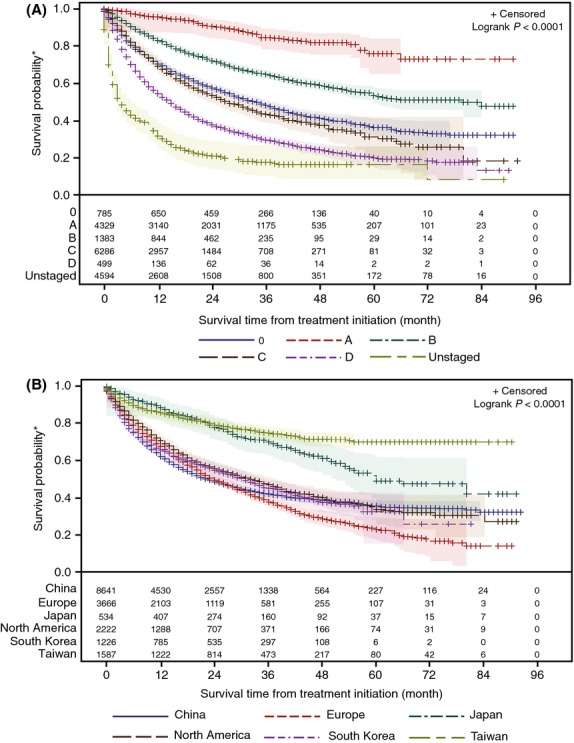
Results: Forty-two sites in 14 countries contributed final data for 18 031 patients. Asia accounted for 67% of patients, Europe for 20% and North America for 13%. As expected, the most common risk factor was hepatitis C virus in North America, Europe and Japan, and hepatitis B virus in China, South Korea and Taiwan. The most common Barcelona Clinic Liver Cancer stage at diagnosis was C in North America, Europe, China and South Korea, and A in Taiwan and Japan. Across all stages, first HCC treatment was most frequently transarterial chemoembolization in North America, Europe, China and South Korea, percutaneous ethanol injection or radiofrequency ablation in Japan and resection in Taiwan. Survival from first HCC treatment varied significantly by region, with median overall survival not reached for Taiwan and 60, 33, 31, 24 and 23 months for Japan, North America, South Korea, Europe and China respectively (P < 0.0001).
Conclusions: Initial results from the BRIDGE study confirm previously reported regional trends in patient demographic characteristics and HCC risk factors, document the heterogeneity of treatment approaches across regions/countries and underscore the need for earlier HCC diagnosis worldwide.
Keywords: disease management; epidemiology; global trends; liver cancer; observational study; risk factors; treatment patterns.
© 2015 The Authors. Liver International Published by John Wiley & Sons Ltd.
Figures



References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0. Estimated cancer incidence, mortality, and prevalence worldwide. Available at http://globocan.iarc.fr. Accessed 28 March 2014.
-
- European Association for The Study Of The Liver; European Organisation for Research And Treatment of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56:908–43. - PubMed
-
- Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet. 2003;362:1907–17. - PubMed
-
- El Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology. 2007;132:2557–76. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
