

Free-breathing, motion-corrected, highly efficient whole heart T2 mapping at 3T with hybrid radial-cartesian trajectory
- PMID: 25753385
- PMCID: PMC4561222
- DOI: 10.1002/mrm.25576
Free-breathing, motion-corrected, highly efficient whole heart T2 mapping at 3T with hybrid radial-cartesian trajectory
Abstract
Purpose: To develop and test a time-efficient, free-breathing, whole heart T2 mapping technique at 3.0T.
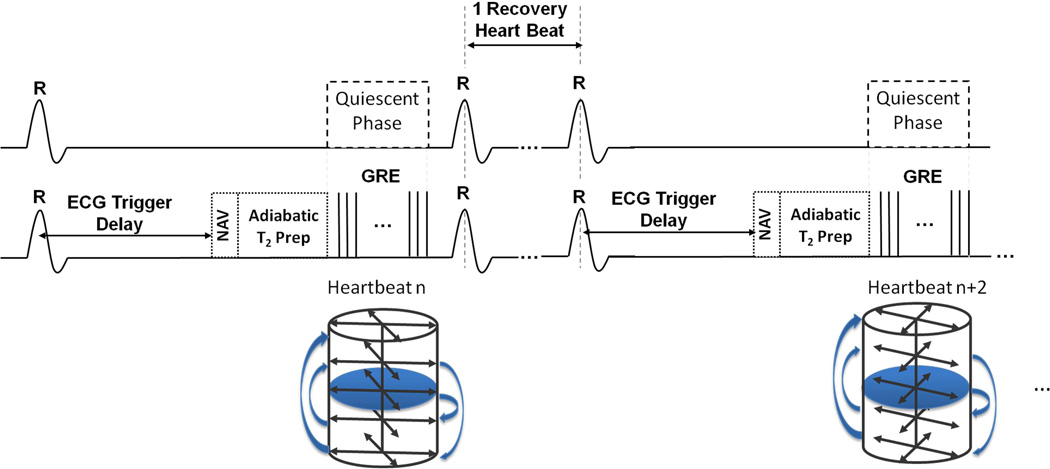
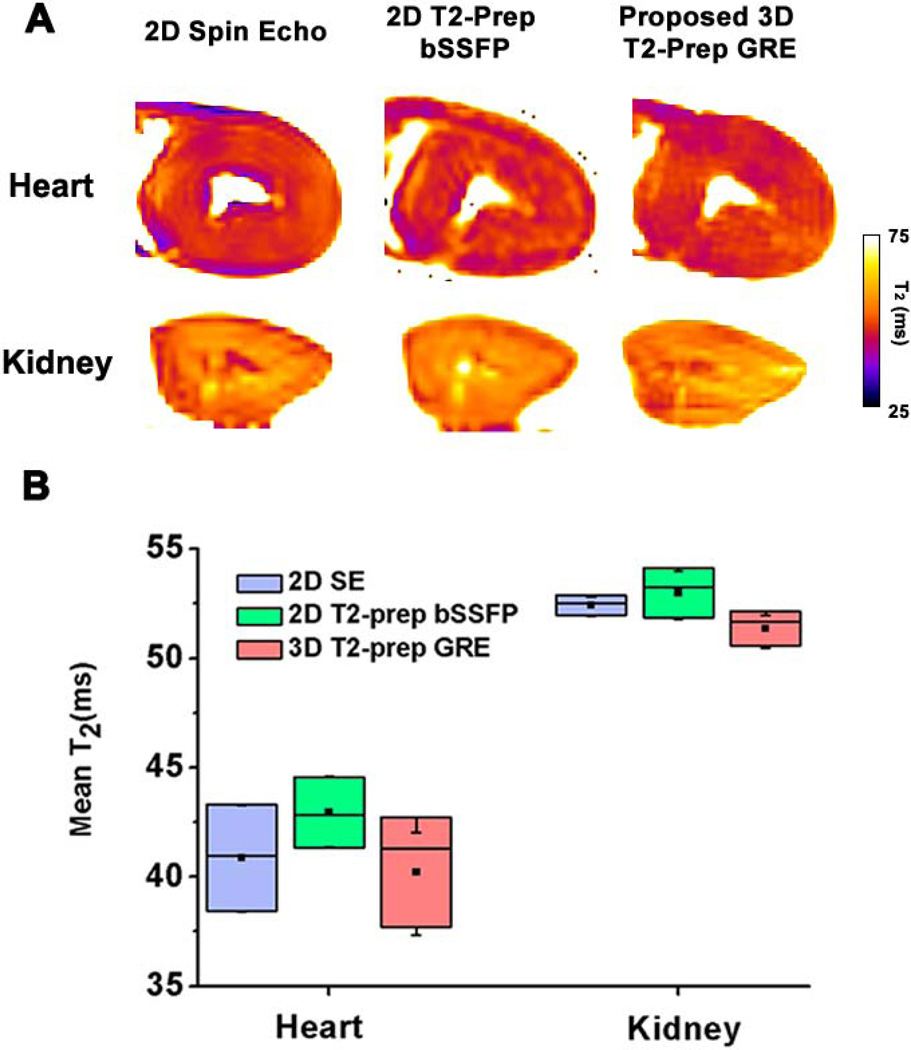
Methods: ECG-triggered three-dimensional (3D) images were acquired with different T2 preparations at 3.0T during free breathing. Respiratory motion was corrected with a navigator-guided motion correction framework at near perfect efficiency. Image intensities were fit to a monoexponential function to derive myocardial T2 maps. The proposed 3D, free breathing, motion-corrected (3D-FB-MoCo) approach was studied in ex vivo canine hearts and kidneys, healthy volunteers, and canine subjects with acute myocardial infarction (AMI).
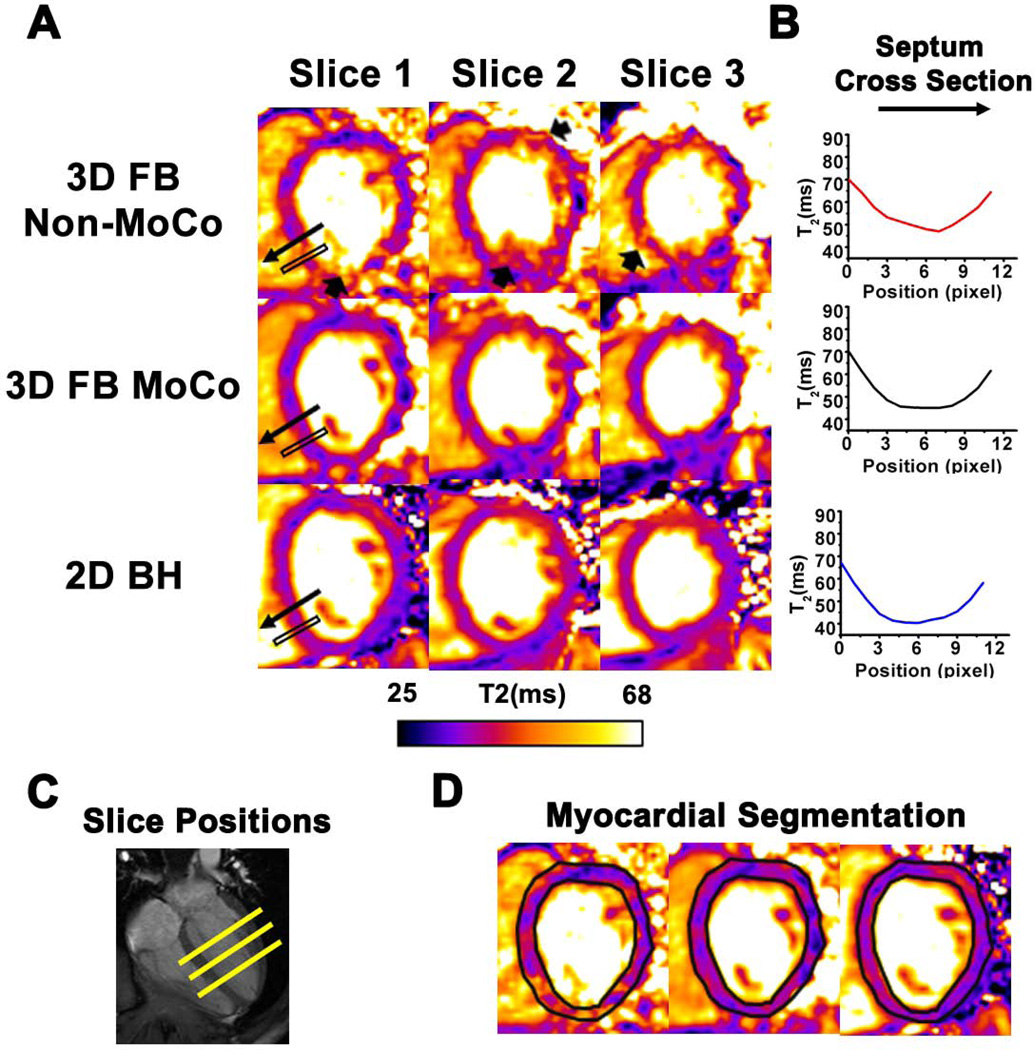
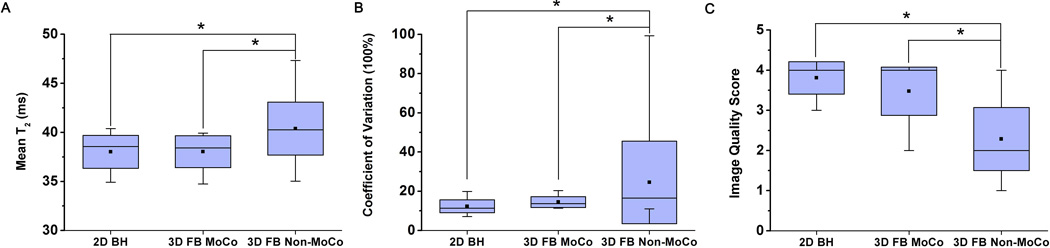
Results: Ex vivo T2 values from proposed 3D T2 -prep gradient echo were not different from two-dimensional (2D) spin echo (P = 0.7) and T2 -prep balanced steady-state free precession (bSSFP) (P = 0.7). In healthy volunteers, compared with 3D-FB-MoCo and breath-held 2D T2 -prep bSSFP (2D-BH), non-motion-corrected (3D-FB-Non-MoCo) myocardial T2 was longer, had a larger coefficient of variation (COV), and had a lower image quality (IQ) score (T2 = 40.3 ms, COV = 38%, and IQ = 2.3; all P < 0.05). Conversely, the mean and COV and IQ of 3D-FB-MoCo (T2 = 37.7 ms, COV = 17%, and IQ = 3.5) and 2D-BH (T2 = 38.0 ms, COV = 15%, and IQ = 3.8) were not different (P = 0.99, P = 0.74, and P = 0.14, respectively). In AMI, T2 values and edema volumes from 3D-FB-MoCo and 2D-BH were closely correlated (R(2) = 0.88 and 0.96, respectively).
Conclusion: The proposed whole heart T2 mapping approach can be performed within 5 min with similar accuracy to that of the 2D-BH T2 mapping approach.
Keywords: cardiac BOLD MRI; cardiac T2 mapping; fast imaging; myocardial edema.
© 2015 Wiley Periodicals, Inc.
Figures


References
-
- Abdel-Aty H, Zagrosek A, Schulz-Menger J, Taylor AJ, Messroghli D, Kumar A, Gross M, Dietz R, Friedrich MG. Delayed enhancement and T2-weighted cardiovascular magnetic resonance imaging differentiate acute from chronic myocardial infarction. Circulation. 2004;109(20):2411–2416. - PubMed
-
- Friedrich MG, Sechtem U, Schulz-Menger J, Holmvang G, Alakija P, Cooper LT, White JA, Abdel-Aty H, Gutberlet M, Prasad S, Aletras A, Laissy JP, Paterson I, Filipchuk NG, Kumar A, Pauschinger M, Liu P. International Consensus Group on Cardiovascular Magnetic Resonance in M. Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. Journal of the American College of Cardiology. 2009;53(17):1475–1487. - PMC - PubMed
-
- Usman AA, Taimen K, Wasielewski M, McDonald J, Shah S, Giri S, Cotts W, McGee E, Gordon R, Collins JD, Markl M, Carr JC. Cardiac magnetic resonance T2 mapping in the monitoring and follow-up of acute cardiac transplant rejection: a pilot study. Circulation Cardiovascular imaging. 2012;5(6):782–790. - PubMed
-
- Payne AR, Casey M, McClure J, McGeoch R, Murphy A, Woodward R, Saul A, Bi X, Zuehlsdorff S, Oldroyd KG, Tzemos N, Berry C. Bright-blood T2-weighted MRI has higher diagnostic accuracy than dark-blood short tau inversion recovery MRI for detection of acute myocardial infarction and for assessment of the ischemic area at risk and myocardial salvage. Circulation Cardiovascular imaging. 2011;4(3):210–219. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
