

Right ventricular function in preterm and term neonates: reference values for right ventricle areas and fractional area of change
- PMID: 25753503
- PMCID: PMC4532398
- DOI: 10.1016/j.echo.2015.01.024
Right ventricular function in preterm and term neonates: reference values for right ventricle areas and fractional area of change
Abstract
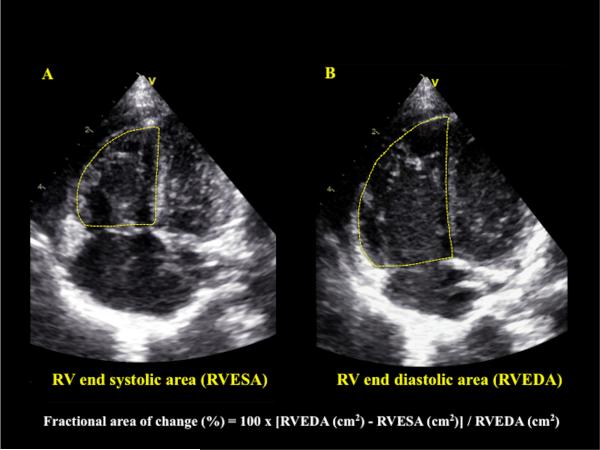
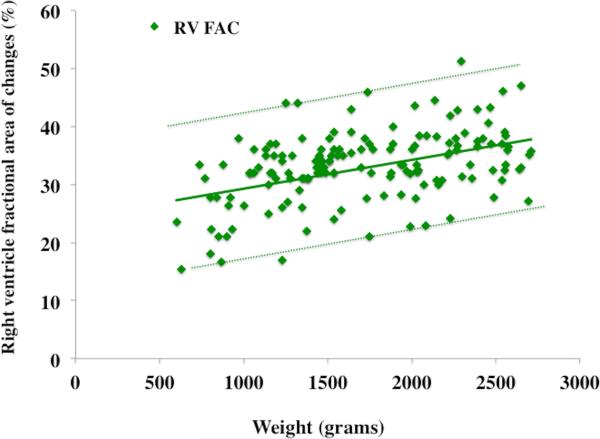
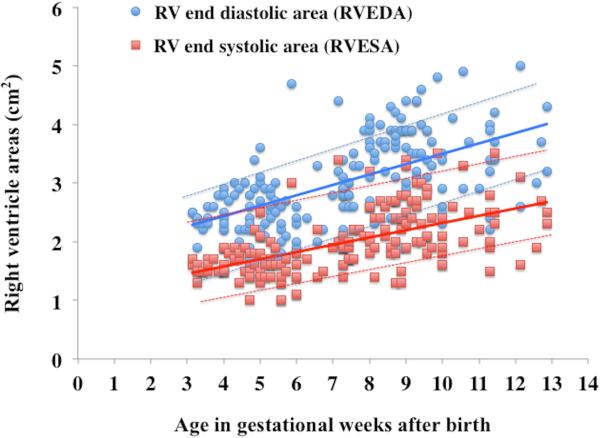
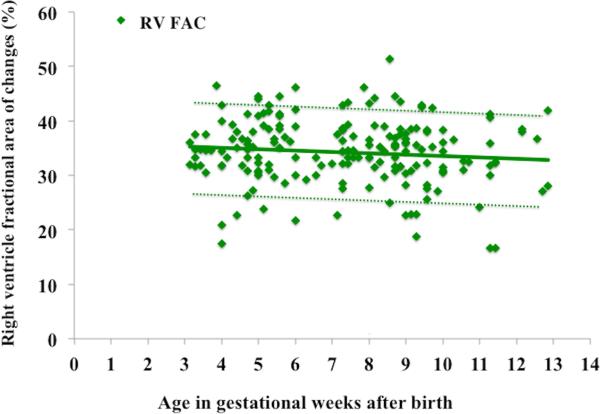
Background: Right ventricular (RV) fractional area of change (FAC) is a quantitative two-dimensional echocardiographic measurement of RV function. RV FAC expresses the percentage change in the RV chamber area between end-diastole (RV end-diastolic area [RVEDA]) to end-systole (RV end-systolic area [RVESA]). The objectives of this study were to determine the maturational (age- and weight-related) changes in RV FAC and RV areas and to establish reference values in healthy preterm and term neonates.
Methods: A prospective longitudinal study was conducted in 115 preterm infants (23-28 weeks' gestational age at birth, 500-1,500 g). RV FAC was measured at 24 hours of age, 72 hours of age, and 32 and 36 weeks' postmenstrual age (PMA). The maturational patterns of RVEDA, RVESA, and RV FAC were compared with those in 60 healthy full-term infants in a cross-sectional study (≥37 weeks, 3.5 ± 1 kg), who underwent echocardiography at birth (n = 25) and 1 month of age (n = 35). RVEDA and RVESA were traced in the RV-focused apical four-chamber view, and FAC was calculated using the formula 100 × [(RVEDA - RVESA)/RVEDA)]. Premature infants who developed chronic lung disease or had clinically and hemodynamically significant patent ductus arteriosus were excluded (n = 55) from the reference values. Intra- and interobserver reproducibility analysis was performed.
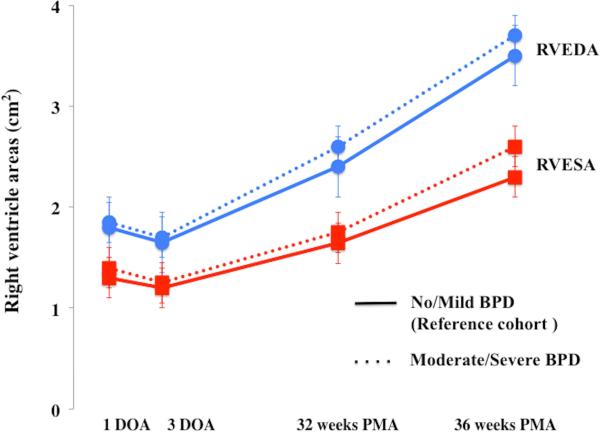
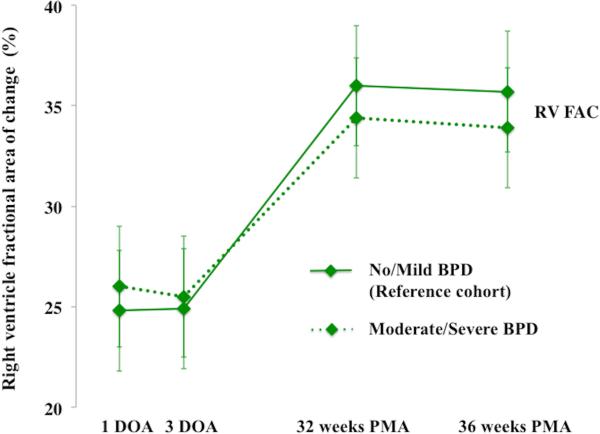
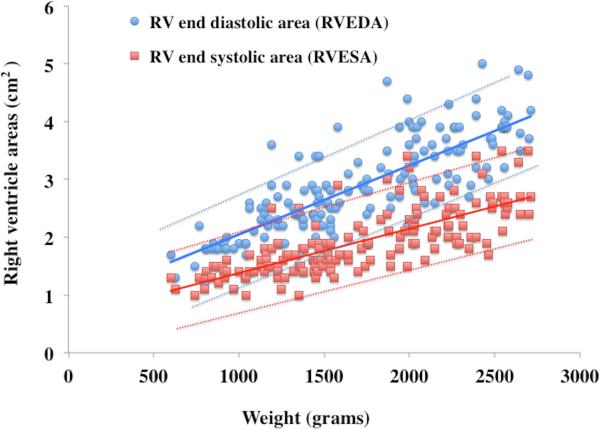
Results: RV FAC ranged from 26% at birth to 35% by 36 weeks' PMA in preterm infants (n = 60) and increased almost 2 times faster in the first month of age compared with healthy term infants (n = 60). Similarly, RVEDA and RVESA increased throughout maturation in both term and preterm infants. RV FAC and RV areas were correlated with weight (r = 0.81, P < .001) but were independent of gestational age at birth (r = 0.3, P = .45). RVEDA and RVESA were correlated with PMA in weeks (r = 0.81, P < .001). RV FAC trended lower in preterm infants with bronchopulmonary dysplasia (P = .04) but was not correlated with size of patent ductus arteriosus (P = .56). There was no difference in RV FAC based on gender or need for mechanical ventilation.
Conclusions: This study establishes reference values of RV areas (RVEDA and RVESA) and RV FAC in healthy term and preterm infants and tracks their maturational changes during postnatal development. These measures increase from birth to 36 weeks' PMA, and this is reflective of the postnatal cardiac growth as a contributor to the maturation of cardiac function These measures are also linearly associated with increasing weight throughout maturation. This study suggests that two-dimensional RV FAC can be used as a complementary modality to assess global RV systolic function in neonates and facilitates its incorporation into clinical pediatric and neonatal guidelines.
Keywords: Cardiac function; Fractional area of change; Neonates; Prematurity; Right ventricle.
Copyright © 2015 American Society of Echocardiography. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Lewandowski AJ, Bradlow WM, Augustine D, Davis EF, Francis J, Singhal A, et al. Right Ventricular Systolic Dysfunction in Young Adults Born Preterm. Circulation. 2013;128:713–20. - PubMed
-
- Rajagopal S, Forsha D, Risum N, Hornik CP, Poms AD, Fortin TA, et al. Comprehensive Assessment of Right Ventricu lar Function in Patients with Pulmonary Hypertension with Global Longitudinal Peak Systolic Strain Derived from Multiple Right Ventricular Views. J Am Soc Echocardiogr. 2014;27:657–65. - PubMed
-
- Jurcut R, Giusca S, La Gerche A, Vasile S, Ginghina C, Voigt JU. The echocardiographic assessment of the right ventricle: what to do in 2010? Eur J Echocardiogr. 2010;11:81–96. - PubMed
-
- Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for chamber quantification. J Am Soc Echocardiogr. 2015;28:1–39. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
