

Improving the outcome for children with cancer: Development of targeted new agents
- PMID: 25754421
- PMCID: PMC4629487
- DOI: 10.3322/caac.21273
Improving the outcome for children with cancer: Development of targeted new agents
Abstract
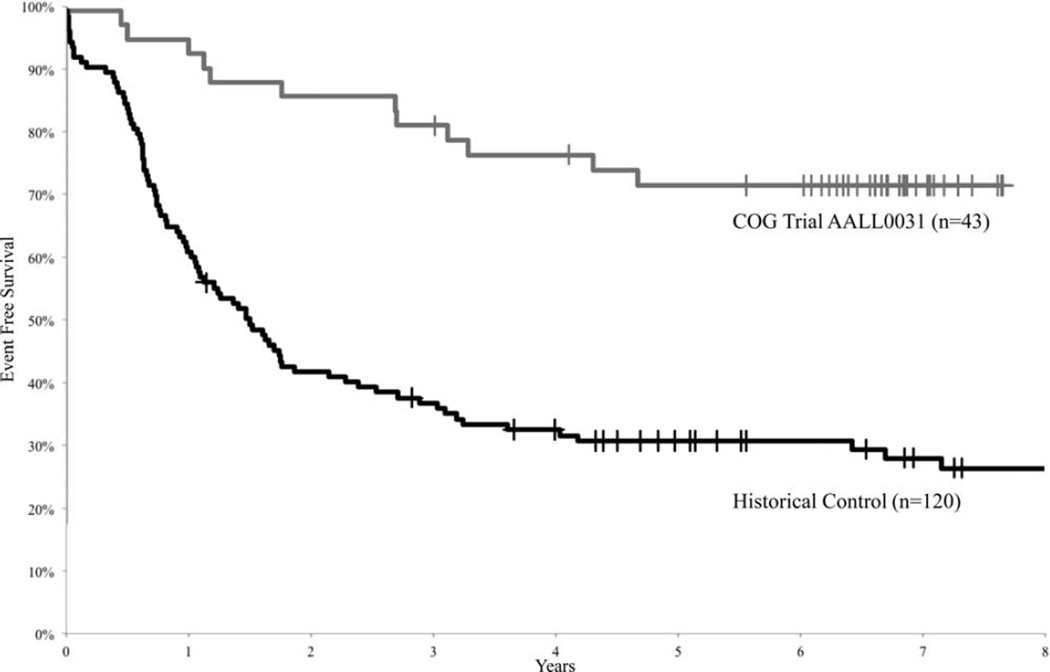
The outcome for children with cancer has improved significantly over the past 60 years, with greater than 80% of patients today becoming 5-year survivors. Despite this progress, cancer remains the leading cause of death from disease in children in the United States, and significant short-term and long-term treatment toxicities continue to impact the majority of children with cancer. The development of targeted new agents offers the prospect of potentially more effective and less toxic treatment for children. More than a decade since imatinib mesylate was introduced into the treatment of children with Philadelphia chromosome-positive acute lymphoblastic leukemia, transforming its outcome, a range of targeted agents has undergone study in pediatric cancer patients. Early lessons learned from these studies include a better understanding of the adverse event profile of these drugs in children, the challenge of developing pediatric-specific formulations, and the continued reliance on successful development for adult cancer indications on pediatric drug development. The collaborative research infrastructure for children with cancer in the United States is well positioned to advance novel treatments into clinical investigations for a spectrum of rare and ultra-rare childhood cancers. A greater investment of resources in target discovery and validation can help drive much needed development of new, more effective treatments for children with cancer.
Keywords: Children's Oncology Group; acute lymphoblastic leukemia; pediatric oncology/hematology; research infrastructure.
© 2015 American Cancer Society.
Figures
Similar articles
-
Collaborative Innovations in Childhood Cancer Therapies.Handb Exp Pharmacol. 2024;286:33-50. doi: 10.1007/164_2024_725. Handb Exp Pharmacol. 2024. PMID: 39177748 Review.
-
Children's clinical cancer trials: what needs to change to allow children access to new cancer drugs?Expert Rev Clin Pharmacol. 2015;8(6):665-7. doi: 10.1586/17512433.2015.1077699. Epub 2015 Aug 24. Expert Rev Clin Pharmacol. 2015. PMID: 26307367
-
New targets and targeted drugs for the treatment of cancer: an outlook to pediatric oncology.Pediatr Hematol Oncol. 2011 Oct;28(7):539-55. doi: 10.3109/08880018.2011.613094. Pediatr Hematol Oncol. 2011. PMID: 21936619 Review.
-
Opportunities and Challenges in Drug Development for Pediatric Cancers.Cancer Discov. 2021 Mar;11(3):545-559. doi: 10.1158/2159-8290.CD-20-0779. Epub 2020 Dec 4. Cancer Discov. 2021. PMID: 33277309 Free PMC article. Review.
-
Targeted approaches to childhood cancer: progress in drug discovery and development.Expert Opin Drug Discov. 2015 May;10(5):483-95. doi: 10.1517/17460441.2015.1025745. Epub 2015 Apr 3. Expert Opin Drug Discov. 2015. PMID: 25840490 Review.
Cited by
-
MyPref: pilot study of a novel communication and decision-making tool for adolescents and young adults with advanced cancer.Support Care Cancer. 2021 Jun;29(6):2983-2992. doi: 10.1007/s00520-020-05806-1. Epub 2020 Oct 8. Support Care Cancer. 2021. PMID: 33030597 Free PMC article.
-
Subsequent Malignant Neoplasm of Bone in Children and Adolescent-Possibility of Multimodal Treatment.Curr Oncol. 2022 Feb 11;29(2):1001-1007. doi: 10.3390/curroncol29020085. Curr Oncol. 2022. PMID: 35200584 Free PMC article.
-
The HIV protease inhibitor, nelfinavir, as a novel therapeutic approach for the treatment of refractory pediatric leukemia.Onco Targets Ther. 2017 May 16;10:2581-2593. doi: 10.2147/OTT.S136484. eCollection 2017. Onco Targets Ther. 2017. PMID: 28553123 Free PMC article.
-
Broad Spectrum Activity of the Checkpoint Kinase 1 Inhibitor Prexasertib as a Single Agent or Chemopotentiator Across a Range of Preclinical Pediatric Tumor Models.Clin Cancer Res. 2019 Apr 1;25(7):2278-2289. doi: 10.1158/1078-0432.CCR-18-2728. Epub 2018 Dec 18. Clin Cancer Res. 2019. PMID: 30563935 Free PMC article.
-
Serum monocyte chemotactic protein 1 and soluble mannose receptor aid predictive diagnosis of pediatric sepsis.Am J Transl Res. 2024 Mar 15;16(3):964-972. doi: 10.62347/FZMM3162. eCollection 2024. Am J Transl Res. 2024. PMID: 38586091 Free PMC article.
References
-
- Hirschfeld S, Ho PT, Smith M, Pazdur R. Regulatory approvals of pediatric oncology drugs: previous experience and new initiatives. J Clin Oncol. 2003;21:1066–1073. - PubMed
-
- Freireich EJ, Kliman A, Gaydos LA, Mantel N, Frei E., 3rd Response to repeated platelet transfusion from the same donor. Ann Intern Med. 1963;59:277–287. - PubMed
-
- Hughes WT, Kuhn S, Chaudhary S, et al. Successful chemoprophylaxis for Pneumocystis carinii pneumonitis. N Engl J Med. 1977;297:1419–1426. - PubMed
-
- Pizzo PA. Infectious complications in the child with cancer. II. Management of specific infectious organisms. J Pediatr. 1981;98:513–523. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
