

Stereotactic radiosurgery for melanoma brain metastases in patients receiving ipilimumab: safety profile and efficacy of combined treatment
- PMID: 25754629
- PMCID: PMC4955924
- DOI: 10.1016/j.ijrobp.2015.01.004
Stereotactic radiosurgery for melanoma brain metastases in patients receiving ipilimumab: safety profile and efficacy of combined treatment
Abstract
Purpose: Ipilimumab (Ipi), a monoclonal antibody against cytotoxic T-lymphocyte antigen-4, has been shown to improve survival in patients with metastatic melanoma. In this single-institution study, we investigated the safety and efficacy of stereotactic radiosurgery (SRS) for patients with melanoma brain metastases (BMs) who also received Ipi.
Methods and materials: From 2005 to 2011, 46 patients with melanoma received Ipi and underwent single-fraction SRS for BMs. A total of 113 BMs (91% intact, 9% postoperative) were treated with a median dose of 21 Gy (range, 15-24 Gy). Ipi was given at 3 mg/kg (54%) or 10 mg/kg (46%) for a median of 4 doses (range, 1-21). Adverse events were recorded with the use of the Common Terminology Criteria for Adverse Events 3.0. Kaplan-Meier methods were used to estimate survival, and Cox regression was used to investigate associations.
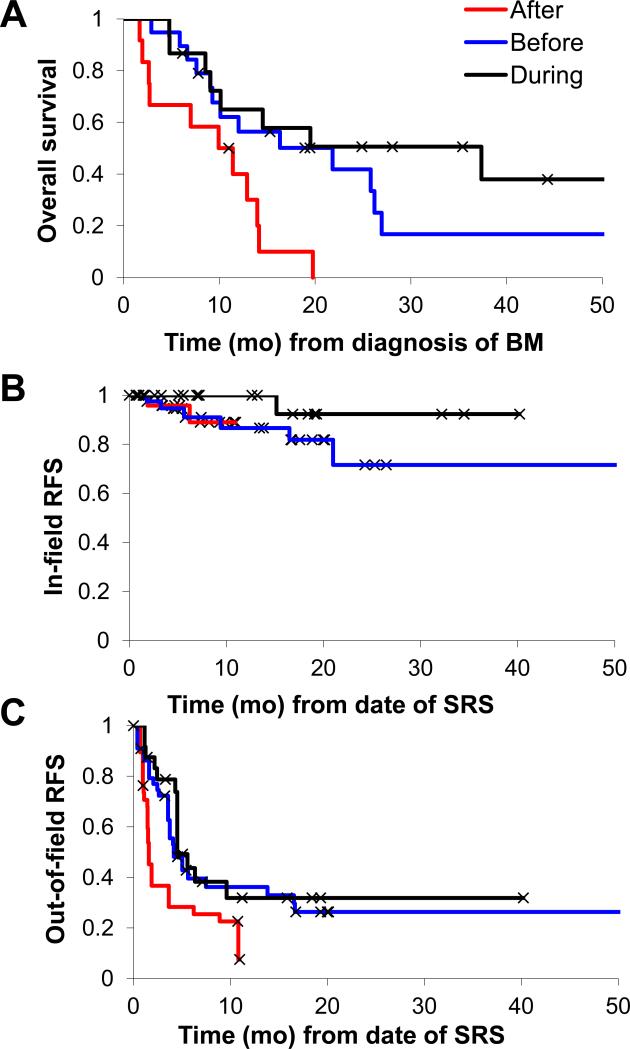
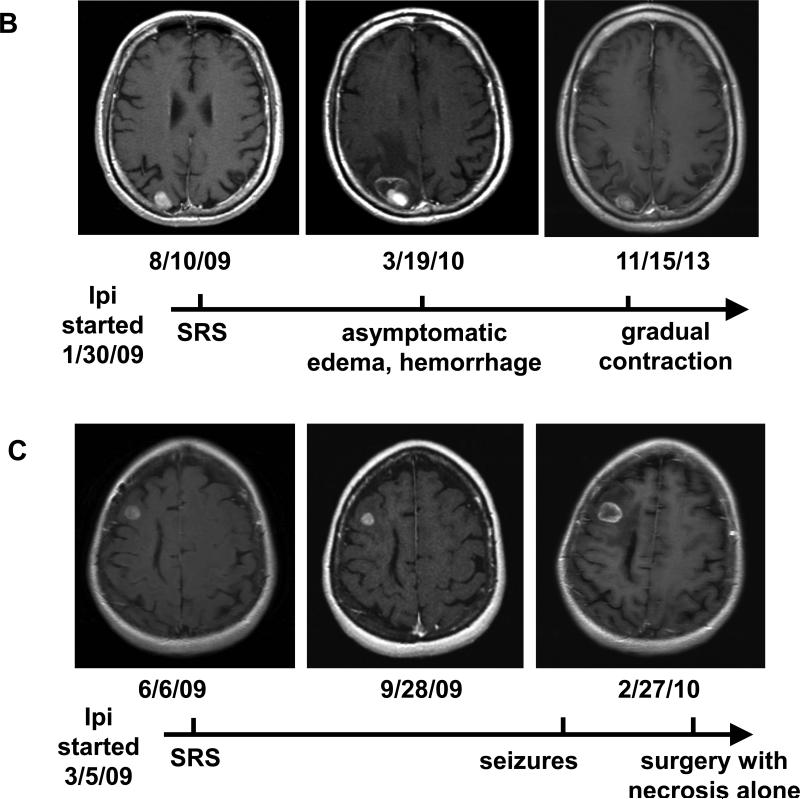
Results: Fifteen patients received SRS during Ipi, 19 received SRS before Ipi, and 12 received SRS after Ipi. Overall survival (OS) was significantly associated with the timing of SRS/Ipi (P=.035) and melanoma-specific graded prognostic assessment (P=.013). Patients treated with SRS during or before Ipi had better OS and less regional recurrence than did those treated with SRS after Ipi (1-year OS 65% vs 56% vs 40%, P=.008; 1-year regional recurrence 69% vs 64% vs 92%, P=.003). SRS during Ipi also yielded a trend toward less local recurrence than did SRS before or after Ipi (1-year local recurrence 0% vs 13% vs 11%, P=.21). On magnetic resonance imaging, an increase in BM diameter to >150% was seen in 50% of patients treated during or before Ipi but in only 13% of patients treated after Ipi. Grade 3 to 4 toxicities were seen in 20% of patients.
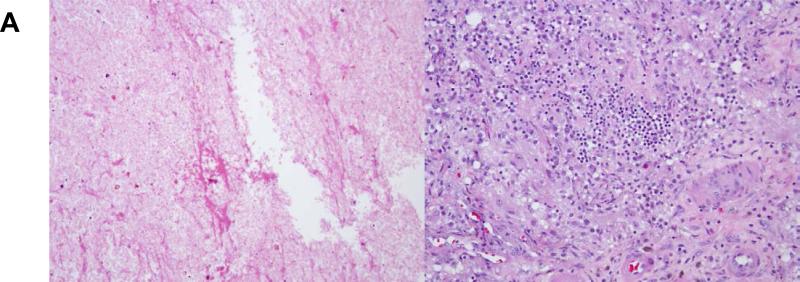
Conclusion: Overall, the combination of Ipi and SRS appears to be well tolerated. Concurrent delivery of Ipi and SRS is associated with favorable locoregional control and possibly longer survival. It may also cause a temporary increase in tumor size, possibly because of an enhanced immunomodulatory effect.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Brain Metastases From Melanoma: Therapy at the Crossroads.Int J Radiat Oncol Biol Phys. 2016 Nov 15;96(4):713-716. doi: 10.1016/j.ijrobp.2016.06.005. Int J Radiat Oncol Biol Phys. 2016. PMID: 27788943 No abstract available.
References
-
- Robert C, Thomas L, Bondarenko I, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011 Jun 30;364(26):2517–2526. - PubMed
-
- Gupta T. Stereotactic radiosurgery for brain oligometastases: good for some, better for all? Ann Oncol. 2005 Nov;16(11):1749–1754. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
