

Early toxicity in patients treated with postoperative proton therapy for locally advanced breast cancer
- PMID: 25754632
- PMCID: PMC4972493
- DOI: 10.1016/j.ijrobp.2015.01.005
Early toxicity in patients treated with postoperative proton therapy for locally advanced breast cancer
Abstract
Purpose: To report dosimetry and early toxicity data in breast cancer patients treated with postoperative proton radiation therapy.
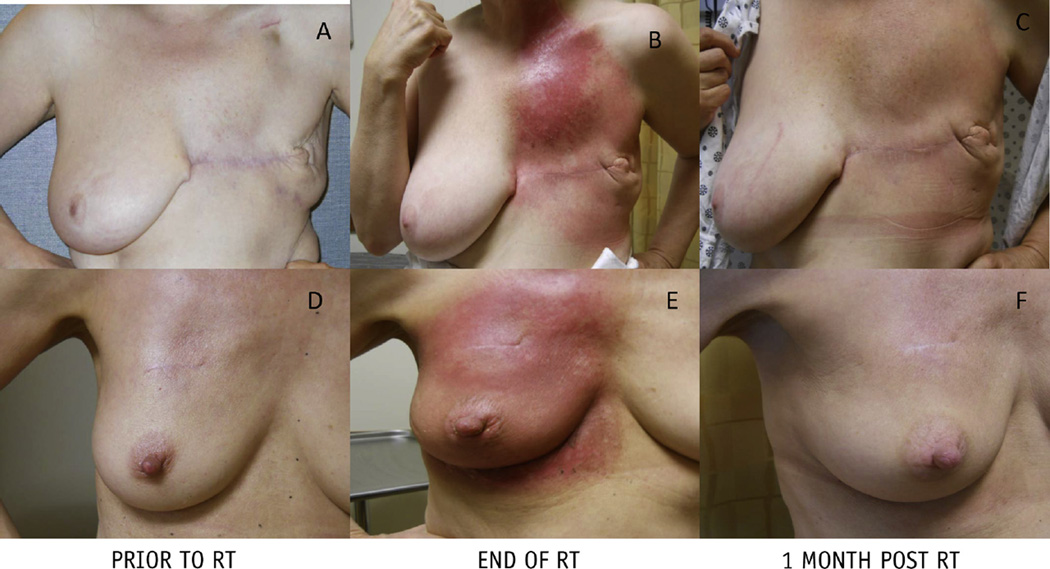
Methods and materials: From March 2013 to April 2014, 30 patients with nonmetastatic breast cancer and no history of prior radiation were treated with proton therapy at a single proton center. Patient characteristics and dosimetry were obtained through chart review. Patients were seen weekly while on treatment, at 1 month after radiation therapy completion, and at 3- to 6-month intervals thereafter. Toxicity was scored using Common Terminology Criteria for Adverse Events version 4.0. Frequencies of toxicities were tabulated.
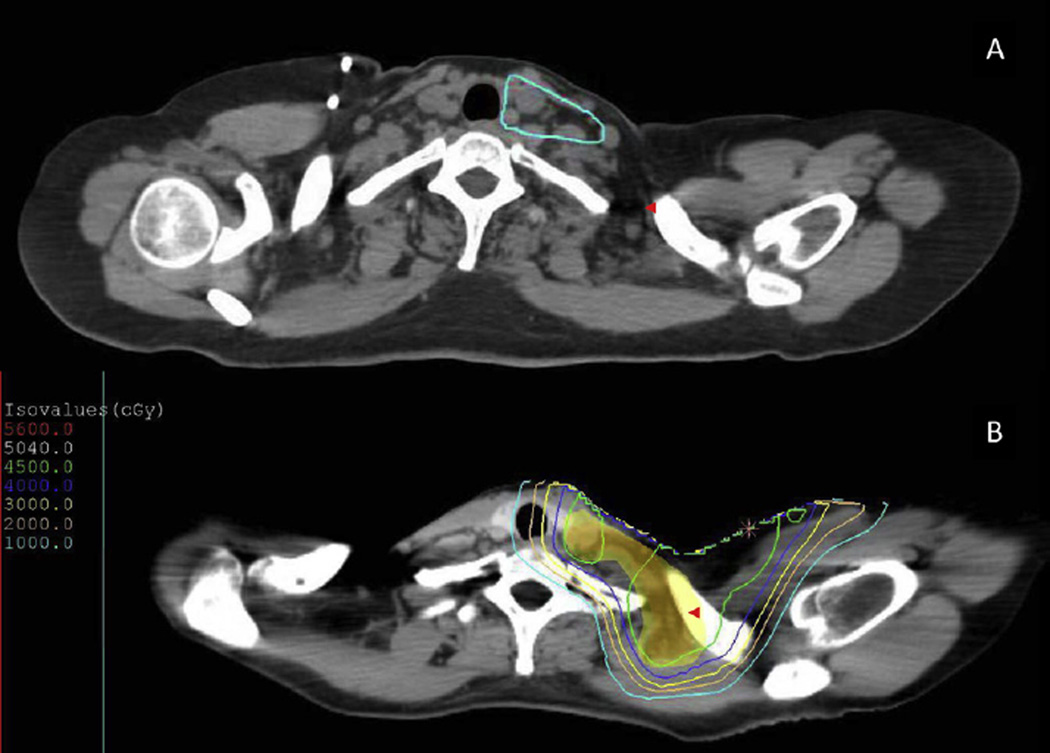
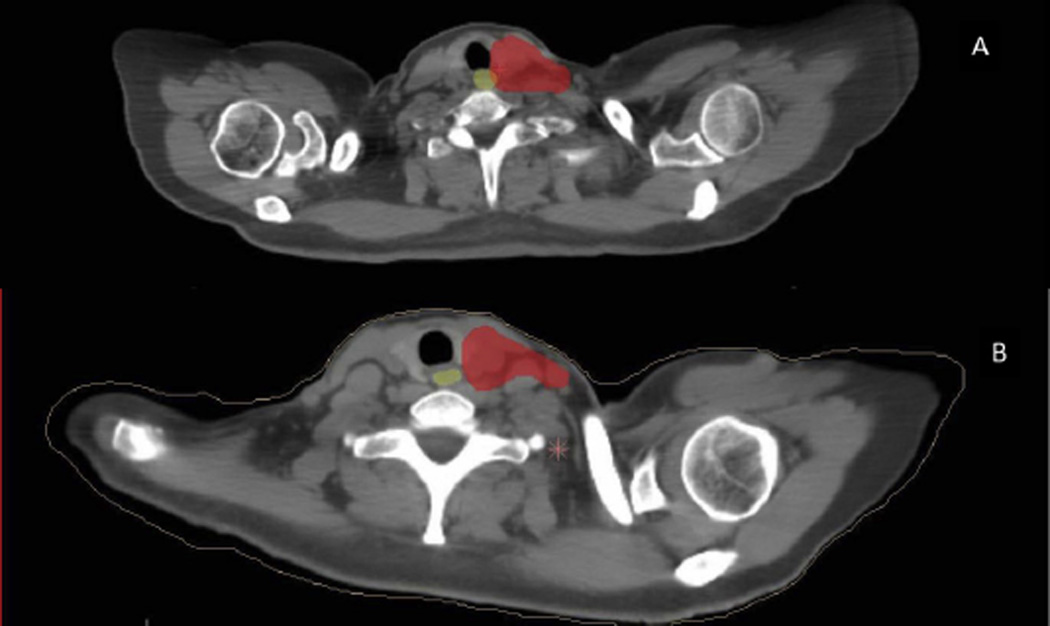
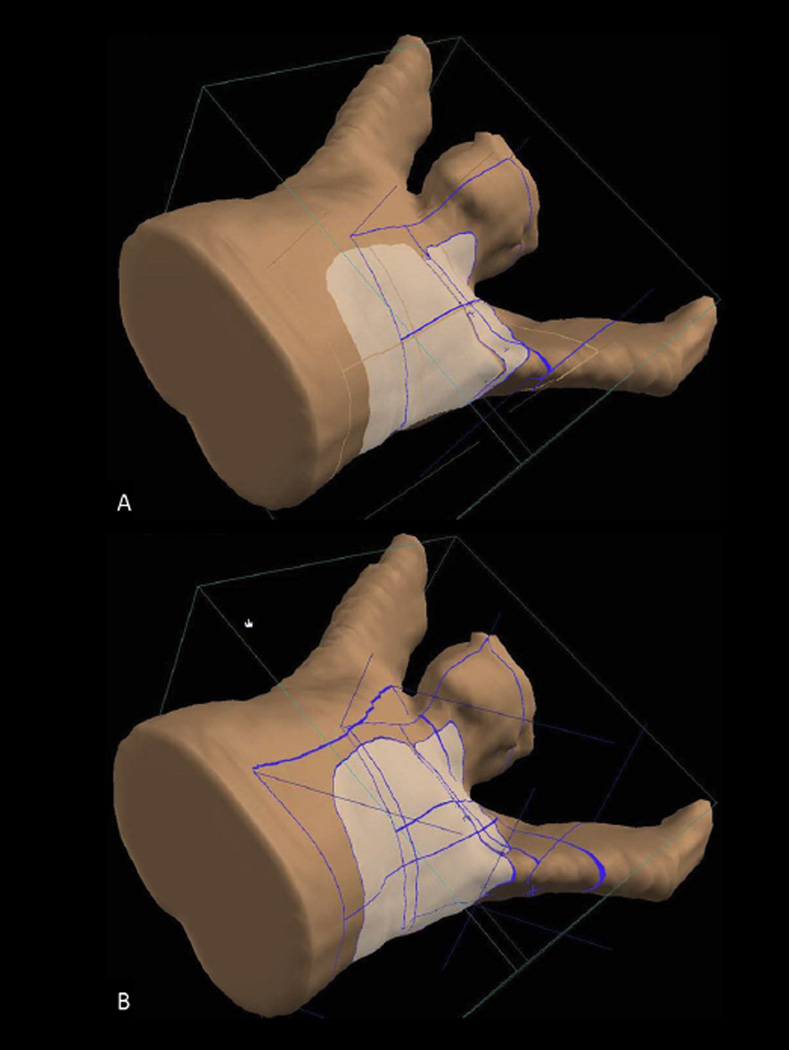
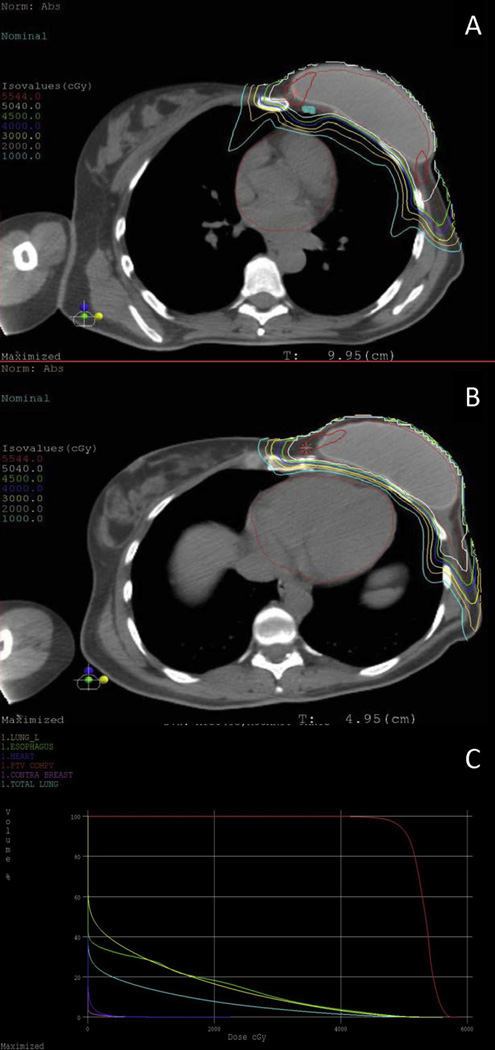
Results: Median dose delivered was 50.4 Gy (relative biological equivalent [RBE]) in 5 weeks. Target volumes included the breast/chest wall and regional lymph nodes including the internal mammary lymph nodes (in 93%). No patients required a treatment break. Among patients with >3 months of follow-up (n=28), grade 2 dermatitis occurred in 20 patients (71.4%), with 8 (28.6%) experiencing moist desquamation. Grade 2 esophagitis occurred in 8 patients (28.6%). Grade 3 reconstructive complications occurred in 1 patient. The median planning target volume V95 was 96.43% (range, 79.39%-99.60%). The median mean heart dose was 0.88 Gy (RBE) [range, 0.01-3.20 Gy (RBE)] for all patients, and 1.00 Gy (RBE) among patients with left-sided tumors. The median V20 of the ipsilateral lung was 16.50% (range, 6.1%-30.3%). The median contralateral lung V5 was 0.34% (range, 0%-5.30%). The median maximal point dose to the esophagus was 45.65 Gy (RBE) [range, 0-65.4 Gy (RBE)]. The median contralateral breast mean dose was 0.29 Gy (RBE) [range, 0.03-3.50 Gy (RBE)].
Conclusions: Postoperative proton therapy is well tolerated, with acceptable rates of skin toxicity. Proton therapy favorably spares normal tissue without compromising target coverage. Further follow-up is necessary to assess for clinical outcomes and cardiopulmonary toxicities.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: B.C., H.T., and O.C. have minority investment in ProCure Proton Therapy Center, Somerset, NJ.
Figures
References
-
- Overgaard M, Hansen PS, Overgaard J, et al. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. Danish Breast Cancer Cooperative Group 82B trial. N Engl J Med. 1997;337:949–955. - PubMed
-
- Overgaard M, Jensen MB, Overgaard J, et al. Postoperative radiotherapy in high-risk postmenopausal breast-cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial. Lancet. 1999;353:1641–1648. - PubMed
-
- Ragaz J, Olivotto IA, Spinelli JJ, et al. Locoregional radiation therapy in patients with high-risk breast cancer receiving adjuvant chemotherapy:20-year results of the British Columbia randomized trial. J Natl Cancer Inst. 2005;97:116–126. - PubMed
-
- Early Breast Cancer Trialists’ Collaborative G. Darby S, McGale P, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011;378:1707–1716. - PMC - PubMed
-
- Whelan TJ, Olivatto I, Ackerman I, et al. NCIC-CTG MA.20: An intergroup trial of regional nodal irradiation in early breast cancer. J Clin Oncol. 2011;29(18 suppl) Abstract LBA 1003.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
