

Heart failure with preserved ejection fraction in the elderly: scope of the problem
- PMID: 25754674
- PMCID: PMC5300019
- DOI: 10.1016/j.yjmcc.2015.02.025
Heart failure with preserved ejection fraction in the elderly: scope of the problem
Abstract
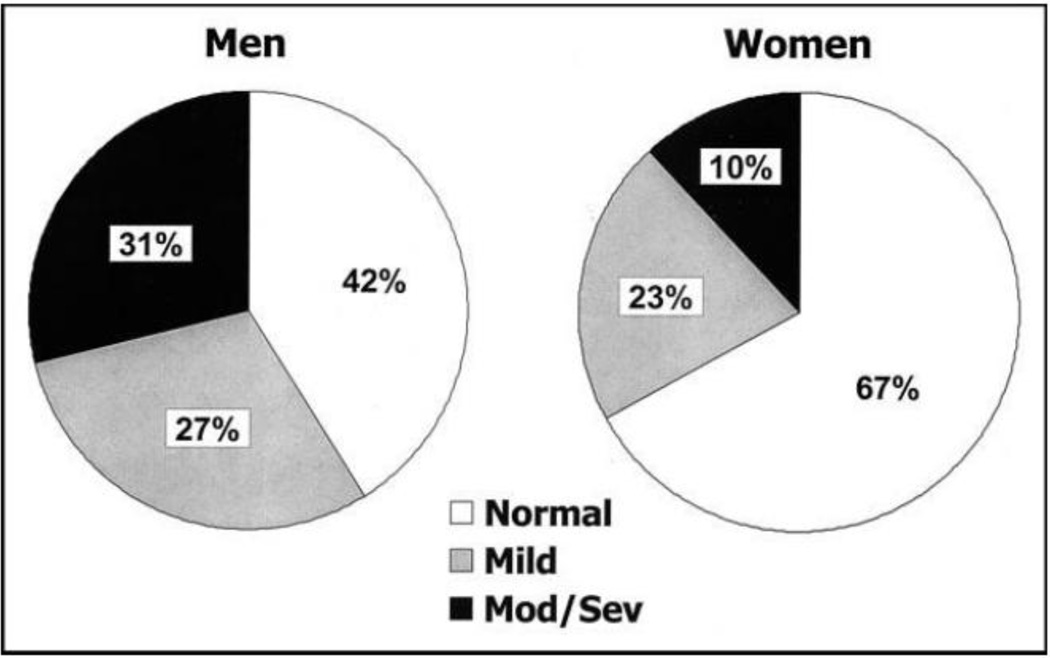
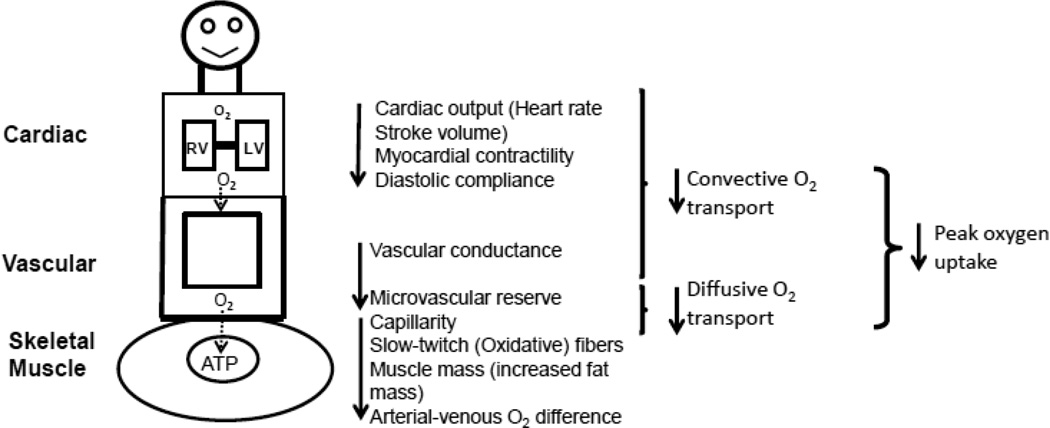
Heart failure with preserved ejection fraction (HFpEF) is the most common form of heart failure (HF) in older adults, particularly women, and is increasing in prevalence as the population ages. With morbidity and mortality on par with HF with reduced ejection fraction, it remains a most challenging clinical syndrome for the practicing clinician and basic research scientist. Originally considered to be predominantly caused by diastolic dysfunction, more recent insights indicate that HFpEF in older persons is typified by a broad range of cardiac and non-cardiac abnormalities and reduced reserve capacity in multiple organ systems. The globally reduced reserve capacity is driven by: 1) inherent age-related changes; 2) multiple, concomitant co-morbidities; 3) HFpEF itself, which is likely a systemic disorder. These insights help explain why: 1) co-morbidities are among the strongest predictors of outcomes; 2) approximately 50% of clinical events in HFpEF patients are non-cardiovascular; 3) clinical drug trials in HFpEF have been negative on their primary outcomes. Embracing HFpEF as a true geriatric syndrome, with complex, multi-factorial pathophysiology and clinical heterogeneity could provide new mechanistic insights and opportunities for progress in management. This article is part of a Special Issue entitled CV Aging.
Keywords: Aging; Heart failure with preserved ejection fraction; Review; Systemic disorder.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
No other members of the writing group have conflicts of interest to declare.
Figures
References
-
- Gottdiener JS, Arnold AM, Aurigemma GP, Polak JF, Tracy RP, Kitzman DW, et al. Predictors of congestive heart failure in the elderly: the Cardiovascular Health Study. J Am Coll Cardiol. 2000;35:1628–1637. - PubMed
-
- Steinberg BA, Zhao X, Heidenreich PA, Peterson ED, Bhatt DL, Cannon CP, et al. Trends in Patients Hospitalized With Heart Failure and Preserved Left Ventricular Ejection Fraction: Prevalence, Therapies, and Outcomes. Circulation. 2012;126:65–75. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006;355:260–269. - PubMed
-
- Liao L, Jollis JG, Anstrom KJ, Whellan DJ, Kitzman DW, Aurigemma GP, et al. Costs for Heart Failure With Normal vs Reduced Ejection Fraction. Arch Intern Med. 2006;166:112–118. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
