

Timeliness of outpatient follow-up: an evidence-based approach for planning after hospital discharge
- PMID: 25755032
- PMCID: PMC4369604
- DOI: 10.1370/afm.1753
Timeliness of outpatient follow-up: an evidence-based approach for planning after hospital discharge
Abstract
Purpose: Timely outpatient follow-up has been promoted as a key strategy to reduce hospital readmissions, though one-half of patients readmitted within 30 days of hospital discharge do not have follow-up before the readmission. Guidance is needed to identify the optimal timing of hospital follow-up for patients with conditions of varying complexity.
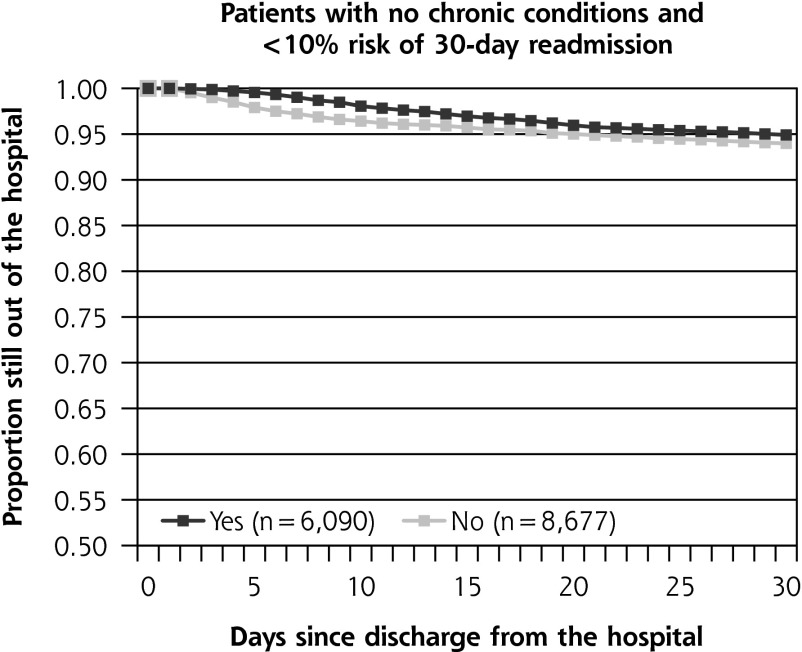
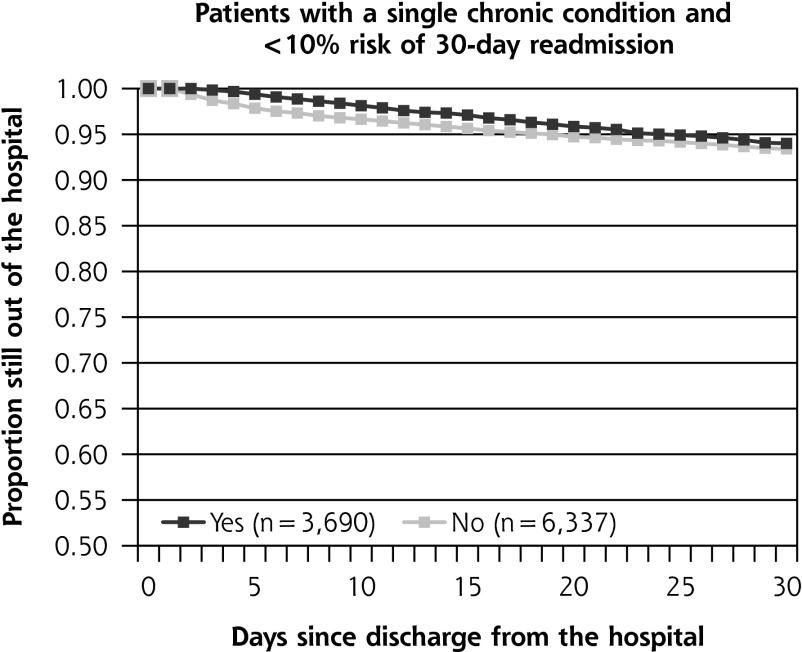
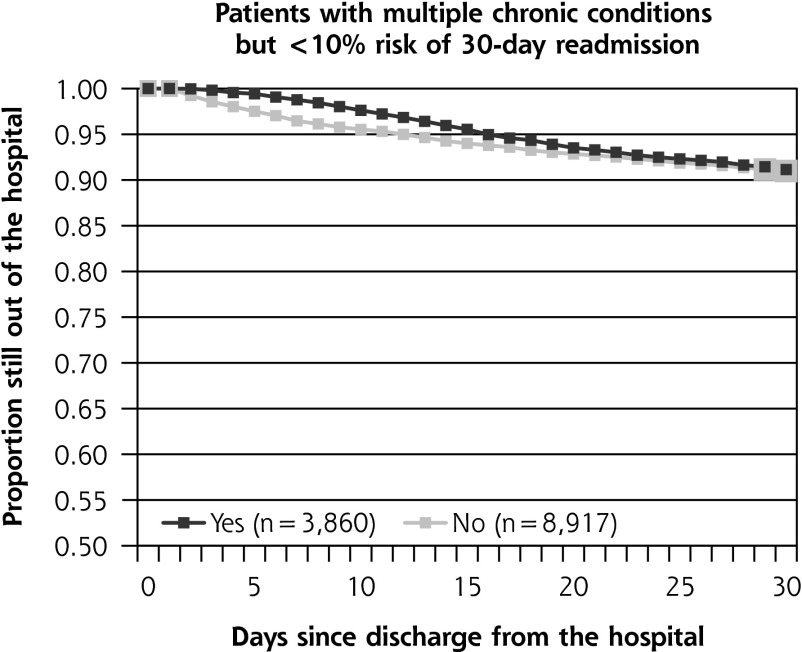
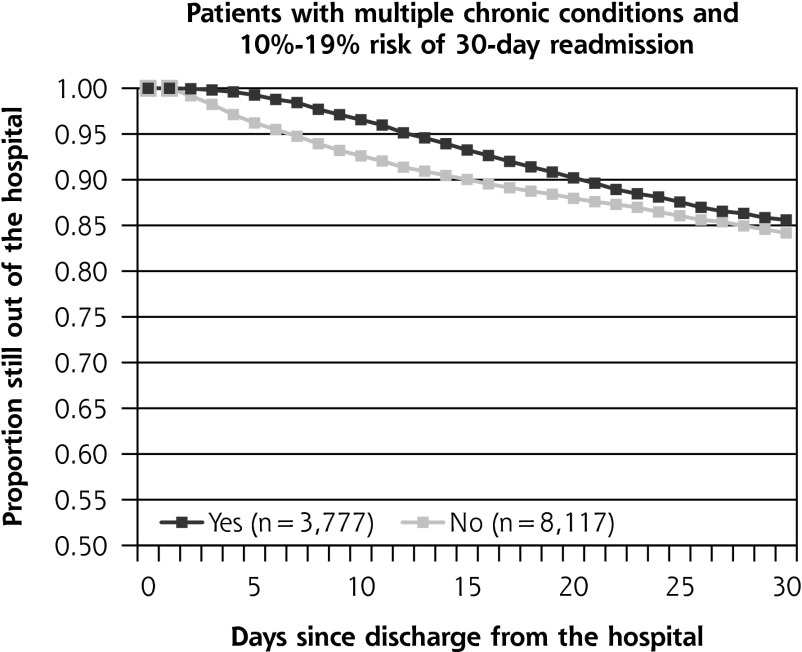
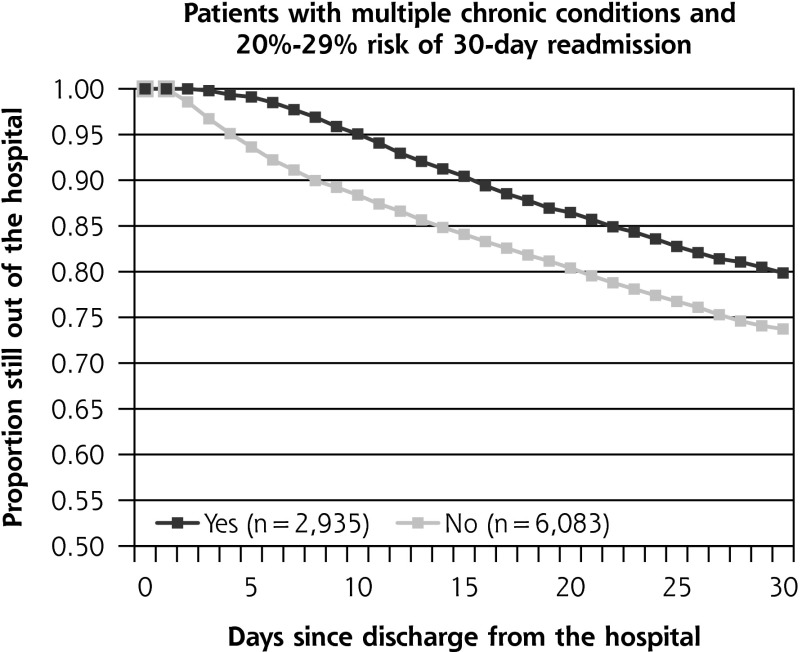
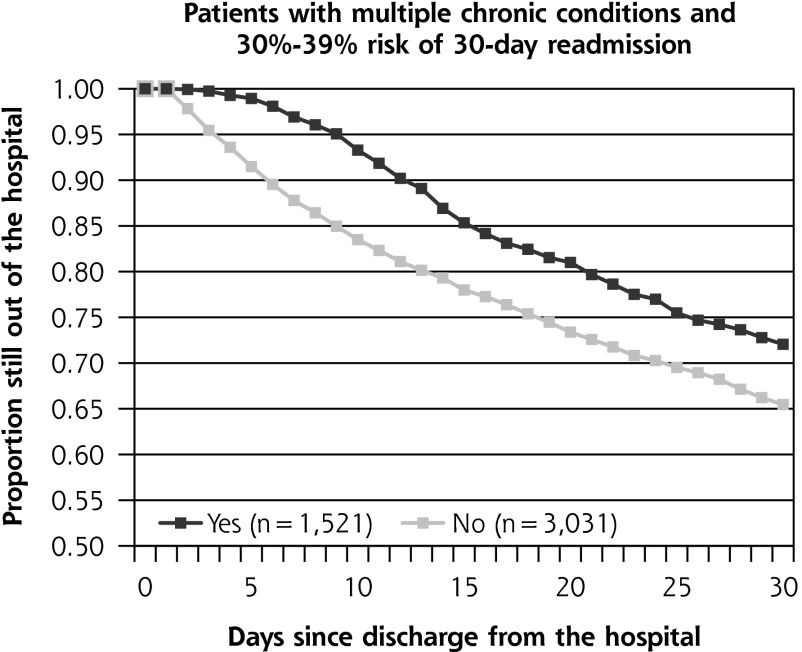
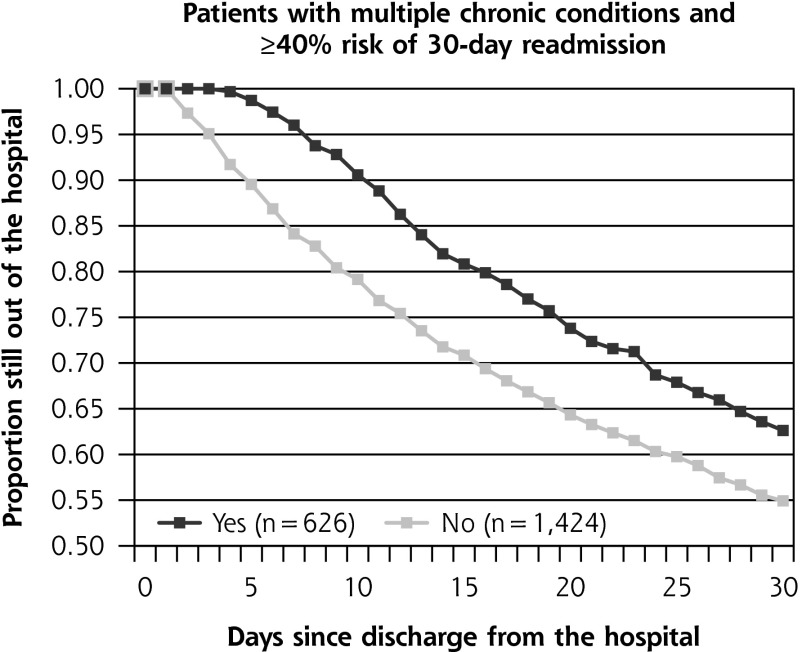
Methods: Using North Carolina Medicaid claims data for hospital-discharged patients from April 2012 through March 2013, we constructed variables indicating whether patients received follow-up visits within successive intervals and whether these patients were readmitted within 30 days. We constructed 7 clinical risk strata based on 3M Clinical Risk Groups (CRGs) and determined expected readmission rates within each CRG. We applied survival modeling to identify groups that appear to benefit from outpatient follow-up within 3, 7, 14, 21, and 30 days after discharge.
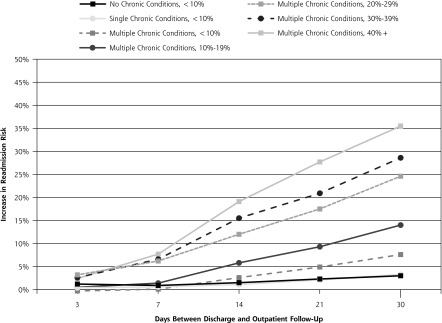
Results: The final study sample included 44,473 Medicaid recipients with 65,085 qualifying discharges. The benefit of early follow-up varied according to baseline readmission risk. For example, follow-up within 14 days after discharge was associated with 1.5%-point reduction in readmissions in the lowest risk strata (P <.001) and a 19.1%-point reduction in the highest risk strata (P <.001). Follow-up within 7 days was associated with meaningful reductions in readmission risk for patients with multiple chronic conditions and a greater than 20% baseline risk of readmission, a group that represented 24% of discharged patients.
Conclusions: Most patients do not meaningfully benefit from early outpatient follow-up. Transitional care resources would be best allocated toward ensuring that highest risk patients receive follow-up within 7 days.
Keywords: chronic disease; continuity of care; hospital readmissions; nursing care management; primary care.
© 2015 Annals of Family Medicine, Inc.
Figures
References
-
- Parry C, Min SJ, Chugh A, Chalmers S, Coleman EA. Further application of the care transitions intervention: results of a randomized controlled trial conducted in a fee-for-service setting. Home Health Care Serv Q. 2009;28(2–3):84–99. - PubMed
-
- Naylor MD, Bowles KH, McCauley KM, et al. High-value transitional care: translation of research into practice. J Eval Clin Pract. ISSN 1365-2753. - PubMed
-
- Clancy CM. Reengineering hospital discharge: a protocol to improve patient safety, reduce costs, and boost patient satisfaction. Am J Med Qual. 2009;24(4):344–346. - PubMed
-
- Coleman E, Williams MV. BOOSTing the hospital discharge. J Hosp Med. 2009;4(4)209–210. - PubMed
-
- James J. Health Policy Brief: Medicare Hospital Readmissions Reduction Program. Health Affairs (Millwood). http://www.healthaf-fairs.org/healthpolicybriefs/brief.php?brief_id=102. Published Nov 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous