

Neonatal hemochromatosis
- PMID: 25755519
- PMCID: PMC3940210
- DOI: 10.1016/j.jceh.2013.10.004
Neonatal hemochromatosis
Abstract
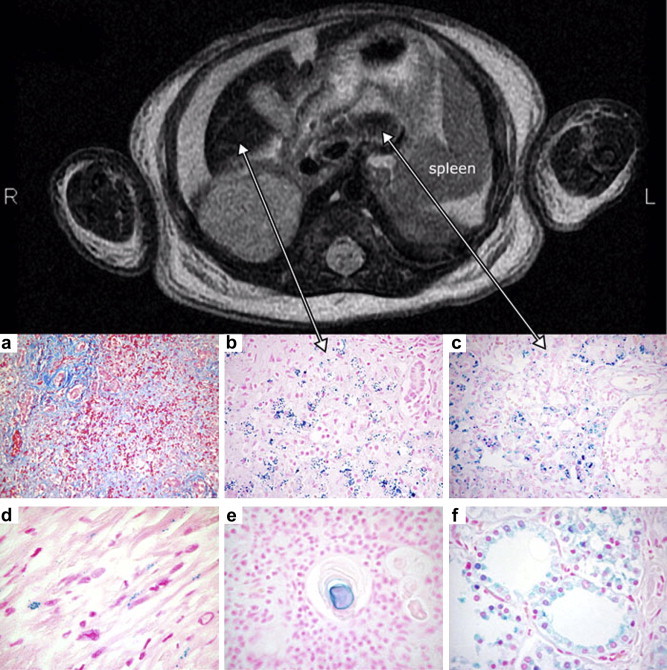
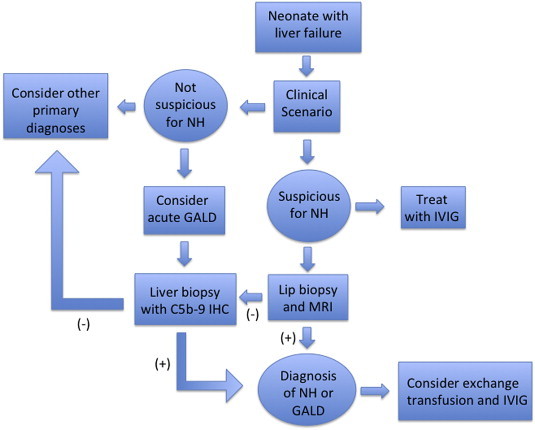
Neonatal hemochromatosis is a clinical condition in which severe liver disease in the newborn is accompanied by extrahepatic siderosis. Gestational alloimmune liver disease (GALD) has been established as the cause of fetal liver injury resulting in nearly all cases of NH. In GALD, a women is exposed to a fetal antigen that she does not recognize as "self" and subsequently begins to produce IgG antibodies that are directed against fetal hepatocytes. These antibodies bind to fetal liver antigen and activate the terminal complement cascade resulting in hepatocyte injury and death. GALD can cause congenital cirrhosis or acute liver failure with and without iron overload and siderosis. Practitioners should consider GALD in cases of fetal demise, stillbirth, and neonatal acute liver failure. Identification of infants with GALD is important as treatment is available and effective for subsequent pregnancies.
Keywords: FcRn, fragment receptor; GALD, gestational alloimmune liver disease; IVIG, intravenous immunoglobulin; IgG, immunoglobulin G; NH, neonatal hemochromatosis; NTBI, non-transferrin bound iron; acute liver failure; complement; gestational alloimmune liver disease; immunoglobulin.
Figures
References
-
- Pan X., Kelly S., Melin-Aldana H., Malladi P., Whitington P.F. Novel mechanism of fetal hepatocyte injury in congenital alloimmune hepatitis involves the terminal complement cascade. Hepatology. Jun 2010;51(6):2061–2068. - PubMed
-
- Knisely A.S., Mieli-Vergani G., Whitington P.F. Neonatal hemochromatosis. Gastroenterol Clin North Am. Sep 2003;32(3):877–889. vi–vii. - PubMed
-
- Whitington P.F., Kelly S. Outcome of pregnancies at risk for neonatal hemochromatosis is improved by treatment with high-dose intravenous immunoglobulin. Pediatrics. Jun 2008;121(6):e1615–1621. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
