

Progressive familial intrahepatic cholestasis
- PMID: 25755532
- PMCID: PMC4017198
- DOI: 10.1016/j.jceh.2013.10.005
Progressive familial intrahepatic cholestasis
Abstract
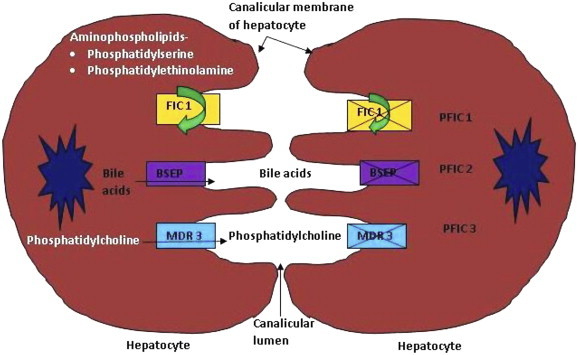
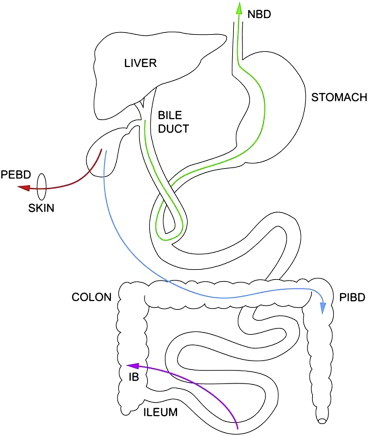
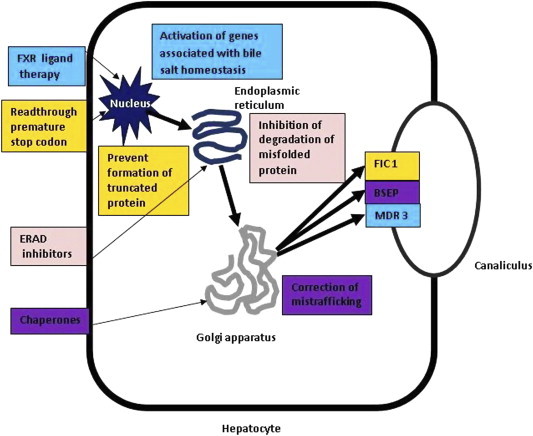
Progressive familial intrahepatic cholestasis (PFIC) is a group of rare disorders which are caused by defect in bile secretion and present with intrahepatic cholestasis, usually in infancy and childhood. These are autosomal recessive in inheritance. The estimated incidence is about 1 per 50,000 to 1 per 100,000 births, although exact prevalence is not known. These diseases affect both the genders equally and have been reported from all geographical areas. Based on clinical presentation, laboratory findings, liver histology and genetic defect, these are broadly divided into three types-PFIC type 1, PFIC type 2 and PFIC type 3. The defect is in ATP8B1 gene encoding the FIC1 protein, ABCB 11 gene encoding BSEP protein and ABCB4 gene encoding MDR3 protein in PFIC1, 2 and 3 respectively. The basic defect is impaired bile salt secretion in PFIC1/2 whereas in PFIC3, it is reduced biliary phospholipid secretion. The main clinical presentation is in the form of cholestatic jaundice and pruritus. Serum gamma glutamyl transpeptidase (GGT) is normal in patients with PFIC1/2 while it is raised in patients with PFIC3. Treatment includes nutritional support (adequate calories, supplementation of fat soluble vitamins and medium chain triglycerides) and use of medications to relieve pruritus as initial therapy followed by biliary diversion procedures in selected patients. Ultimately liver transplantation is needed in most patients as they develop progressive liver fibrosis, cirrhosis and end stage liver disease. Due to the high risk of developing liver tumors in PFIC2 patients, monitoring is recommended from infancy. Mutation targeted pharmacotherapy, gene therapy and hepatocyte transplantation are being explored as future therapeutic options.
Keywords: ABC, ATP binding cassette; ASBT, apical sodium bile salt transporter; ATP, adenosine triphosphate; ATPase, adenosine triphosphatase; BRIC, benign recurrent intrahepatic cholestasis; BSEP, bile salt exporter protein; CFTR, cystic fibrosis transmembrane conductance regulator; CYP, cytochrome P; DNA, deoxyribonucleic acid; ERAD, endoplasmic reticulum associated degradation; ESLD, end stage liver disease; FIC1, familial intrahepatic cholestasis protein 1; FXR, farnesoid X receptor; HCC, hepatocellular carcinoma; IB, ileal bypass; ICP, intrahepatic cholestasis of pregnancy; LT, liver transplant; MARS, Molecular Adsorbent Recirculating System; MDR, multidrug resistance protein; MRCP, magnetic resonance cholangiopancreaticography; PBD, partial biliary drainage; PEBD, partial external biliary drainage; PFIC, progressive familial intrahepatic cholestasis; PIBD, partial internal biliary drainage; PPAR, peroxisome proliferator activator receptor; UDCA, ursodeoxycholic acid; bile secretion; children; cholestasis; familial; mRNA, messenger ribonucleic acid; pGp, p-glycoprotein; pruritus.
Figures
References
-
- Jacquemin E. Progressive familial intrahepatic cholestasis. Clin Res Hepatol Gastroenterol. 2012;36(suppl 1):S26–S35. - PubMed
-
- Hori T., Nguyen J.H., Uemoto S. Progressive familial intrahepatic cholestasis. Hepatobiliary Pancreat Dis Int. 2010;9:570–578. - PubMed
-
- Clayton R.J., Iber F.I., Ruebner B.H. Byler disease: fatal familial intrahepatic cholestasis in an Amish kindred. Am J Dis Child. 1969;117:112–124. - PubMed
-
- Bull L.N., Carlton V.E., Stricker N.L. Genetic and morphological findings in progressive familial intrahepatic cholestasis (Byler disease [PFIC 1] and Byler syndrome): evidence for heterogenicity. Hepatology. 1997;26:155–164. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
