

Portal cavernoma cholangiopathy: consensus statement of a working party of the Indian national association for study of the liver
- PMID: 25755591
- PMCID: PMC4274351
- DOI: 10.1016/j.jceh.2014.02.003
Portal cavernoma cholangiopathy: consensus statement of a working party of the Indian national association for study of the liver
Abstract
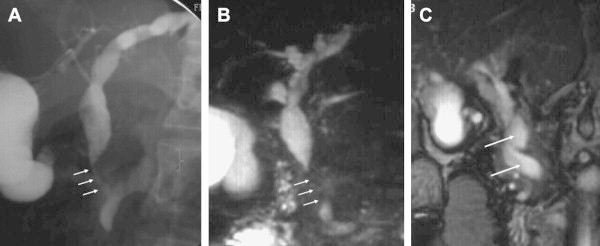
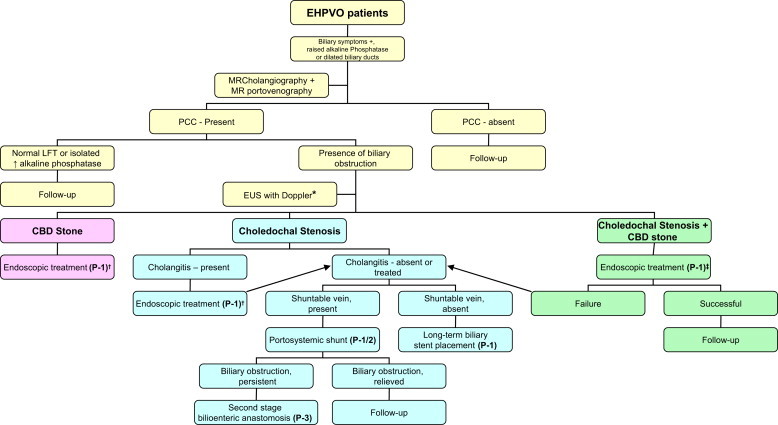
Portal cavernoma cholangiopathy (PCC) is defined as abnormalities in the extrahepatic biliary system including the cystic duct and gallbladder with or without abnormalities in the 1st and 2nd generation biliary ducts in a patient with portal cavernoma. Presence of a portal cavernoma, typical cholangiographic changes on endoscopic or magnetic resonance cholangiography and the absence of other causes of these biliary changes like bile duct injury, primary sclerosing cholangitis, cholangiocarcinoma etc are mandatory to arrive a diagnosis. Compression by porto-portal collateral veins involving the paracholedochal and epicholedochal venous plexuses and cholecystic veins and ischemic insult due to deficient portal blood supply or prolonged compression by collaterals bring about biliary changes. While the former are reversible after porto-systemic shunt surgery, the latter are not. Majority of the patients with PCC are asymptomatic and approximately 21% are symptomatic. Symptoms in PCC could be in the form of long standing jaundice due to chronic cholestasis, or biliary pain with or without cholangitis due to biliary stones. Endoscopic retrograde cholangiography has no diagnostic role because it is invasive and is associated with risk of complications, hence it is reserved for therapeutic procedures. Magnetic resonance cholangiography and portovenography is a noninvasive and comprehensive imaging technique, and is the modality of choice for mapping of the biliary and vascular abnormalities in these patients. PCC is a progressive condition and symptoms develop late in the course of portal hypertension only in patients with severe or advanced changes of cholangiopathy. Asymptomatic patients with PCC do not require any treatment. Treatment of symptomatic PCC can be approached in a phased manner, coping first with biliary clearance by nasobiliary or biliary stent placement for acute cholangitis and endoscopic biliary sphincterotomy for biliary stone removal; second, with portal decompression by creating portosystemic shunt; and third, with persistent biliary obstruction by performing second-stage biliary drainage surgery such as hepaticojejunostomy or choledochoduodenostomy. Patients with symptomatic PCC have good prognosis after successful endoscopic biliary drainage and after successful shunt surgery.
Keywords: CBD, common bile duct; CHD, common hepatic duct; CT, computed tomography; EHPVO, extrahepatic portal venous obstruction; ERC, endoscopic retrograde cholangiography; EUS, endoscopic ultrasound; GRADE, Grading of Recommendations, Assessment, Development and Evaluation; INASL, Indian National Association for Study of the Liver; MRC, magnetic resonance cholangiography; MRI, magnetic resonance imaging; NCPF, non-cirrhotic portal fibrosis; PSS, portosystemic shunt; PVT, portal vein thrombosis; UDCA, ursodeoxycholic acid; USG, ultrasound; cholestasis; extrahepatic portal venous obstruction; gallbladder varices; obstructive jaundice; portal hypertensive biliopathy.
Figures
References
-
- Fraser J., Brown A.K. A clinical syndrome associated with a rare anomaly of vena portal system. Surg Gynecol Obstet. 1944;78:520–524.
-
- Malkan G.H., Bhatia S.J., Bashir K. Cholangiopathy associated with portal hypertension: diagnostic evaluation and clinical implications. Gastrointest Endosc. 1999;49:344–348. - PubMed
-
- Dhiman R.K., Chawla Y., Vasishta R.K. Non-cirrhotic portal fibrosis (idiopathic portal hypertension): experience with 151 patients and a review of the literature. J Gastroenterol Hepatol. 2002;17:6–16. - PubMed
-
- Chandra R., Kapoor D., Tharakan A. Portal biliopathy. J Gastroenterol Hepatol. 2001;16:1086–1092. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
