

Imaging of portal cavernoma cholangiopathy
- PMID: 25755595
- PMCID: PMC4244824
- DOI: 10.1016/j.jceh.2013.07.004
Imaging of portal cavernoma cholangiopathy
Abstract
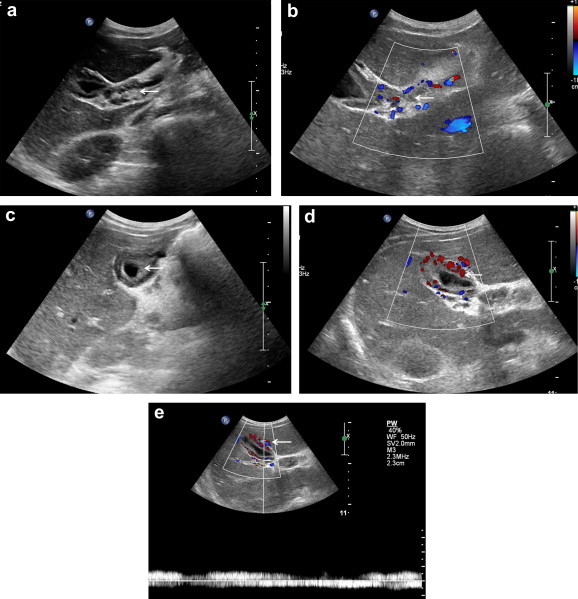
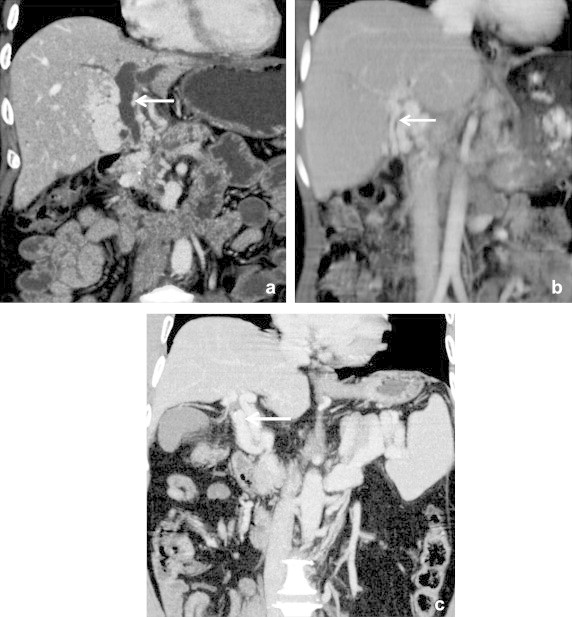
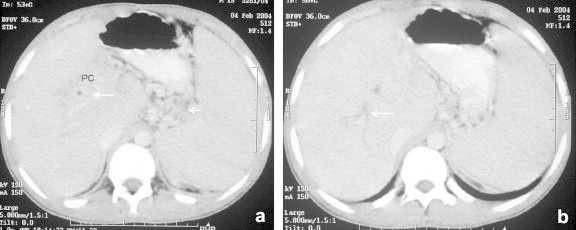
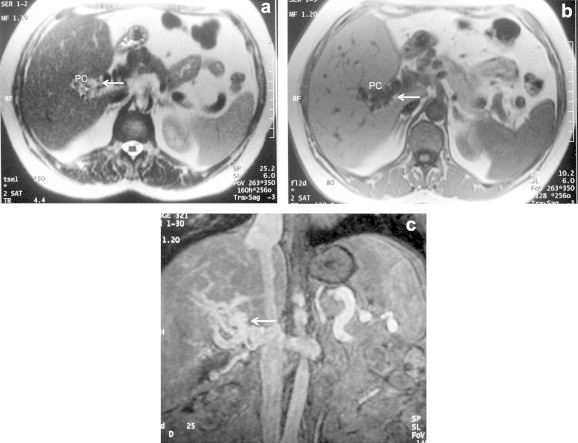
Portal cavernoma cholangiopathy (PCC) refers to the biliary changes which occur in the setting of extrahepatic portal vein obstruction and secondary portal cavernoma formation. The main radiological findings include the vascular changes in the form of portosystemic collaterals and biliary changes in the form of extrinsic impressions and strictures. Till date, conventional cholangiography has been the gold standard for the diagnosis of PCC. However, it is an invasive procedure and is associated with complications. At present there is a transition towards non-invasive modalities like ultrasound (US), computed tomography (CT) and magnetic resonance imaging (MRI). The recent advances in these modalities provide an excellent delineation of both the vascular and the biliary changes non-invasively in a short time. The findings of PCC using these newer modalities are not so well described in literature. The findings of PCC also overlap with malignant conditions of biliary tract such as cholangiocarcinoma and compression of biliary tract by malignant adenopathies. In this article we describe the vascular and biliary changes associated with PCC on US, CT and MRI. We also describe the imaging findings using each modality along with their advantages and disadvantages.
Keywords: CBD, common bile duct; CEMR, contrast enhanced MR; CT, computed tomography; EHPVO, extrahepatic portal vein obstruction; ERCP, endoscopic retrograde cholangiopancreatography; MRI, magnetic resonance imaging; PC, periportal collateral; PC, portal cavernoma; PCC, portal cavernoma cholangiopathy; US, ultrasound; extrahepatic portal vein obstruction; imaging; portal cavernoma cholangiopathy.
Figures


References
-
- Walser E.M., Runyan B.R., Heckman M.G. Extrahepatic portal biliopathy: proposed etiology on the basis of anatomic and clinical features. Radiology. 2011;258:146–153. - PubMed
-
- Valla D., Casadevall N., Huisse M.G. Etiology of portal vein thrombosis in adults. A prospective evaluation of primary myeloproliferative disorders. Gastroenterology. 1988;94:1063–1069. - PubMed
-
- Khuroo M.S., Yattoo G.N., Zargar S.A. Biliary abnormalities associated with extrahepatic portal vein obstruction. Hepatology. 1993;17:807–813. - PubMed
-
- Nagi B., Kochhar R., Bhasin D., Singh K. Cholangiopathy in extrahepatic portal venous obstruction: radiological appearances. Acta Radiol. 2000;41:612–615. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
