

Natural history of portal cavernoma cholangiopathy
- PMID: 25755597
- PMCID: PMC4244826
- DOI: 10.1016/j.jceh.2013.08.003
Natural history of portal cavernoma cholangiopathy
Abstract
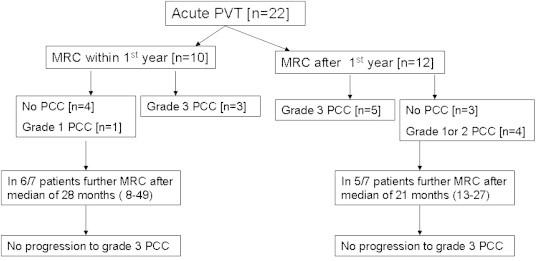
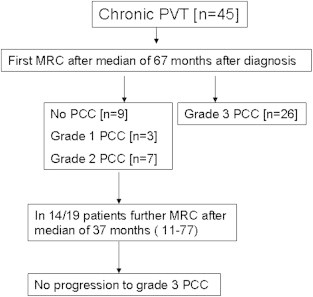
The natural history of portal cavernoma cholangiopathy (PCC) is poorly defined and poorly understood. It develops early after acute portal vein thrombosis (PVT) if there is failure of recanalization. In PCC, the likelihood of progression of biliary abnormalities after 1 year is extremely low. The natural history of PCC is conveniently divided into asymptomatic and symptomatic stages. The majority of patients with PCC are asymptomatic and are detected incidentally on imaging. Limited data suggest that asymptomatic PCC is static or only slowly progressive in the initial stages. However, most workers agree that, overall, PCC is a slowly progressive disease. Symptomatic PCC represents a late stage in its natural history. Finding strictures with dilatation at cholangiography is associated with a higher risk of developing symptoms of PCC. Onset of symptoms is often precipitated by the development of biliary sludge or calculi and treating calculi usually relieves symptoms for prolonged periods of time. Clinical presentations include biliary pain, obstructive jaundice, acute cholangitis, acute cholecystitis, or other presentations of gallstone disease. Progressive liver dysfunction and secondary biliary cirrhosis can develop in a minority of patients.
Keywords: EHPVO, extra-hepatic portal venous obstruction; NCPF, non-cirrhotic portal fibrosis; NCPH, non-cirrhotic portal hypertension; PCC, cavernoma cholangiopathy; PH, portal hypertension; PVCT, portal vein cavernomatous transformation; PVT, portal vein thrombosis; extrahepatic portal venous obstruction; natural history; portal cavernoma cholangiopathy; prognosis.
Figures
References
-
- Poddar U., Borkar V. Management of extra hepatic portal venous obstruction (EHPVO): current strategies. Trop Gastroenterol. 2011;32(2):94–102. - PubMed
-
- Dhiman R.K., Chawla Y., Vasishta R.K. Non-cirrhotic portal fibrosis (idiopathic portal hypertension): experience with 151 patients and a review of the literature. J Gastroenterol Hepatol. 2002;17:6–16. - PubMed
-
- Bayraktar Y., Balkanci F., Kayhan B., Ozenç A., Arslan S., Telatar H. Bile duct varices or “pseudo-cholangiocarcinoma sign” in portal hypertension due to cavernous transformation of the portal vein. Am J Gastroenterol. 1992;87:1801–1806. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
