

Management of BRAF and MEK inhibitor toxicities in patients with metastatic melanoma
- PMID: 25755684
- PMCID: PMC4346212
- DOI: 10.1177/1758834014566428
Management of BRAF and MEK inhibitor toxicities in patients with metastatic melanoma
Abstract
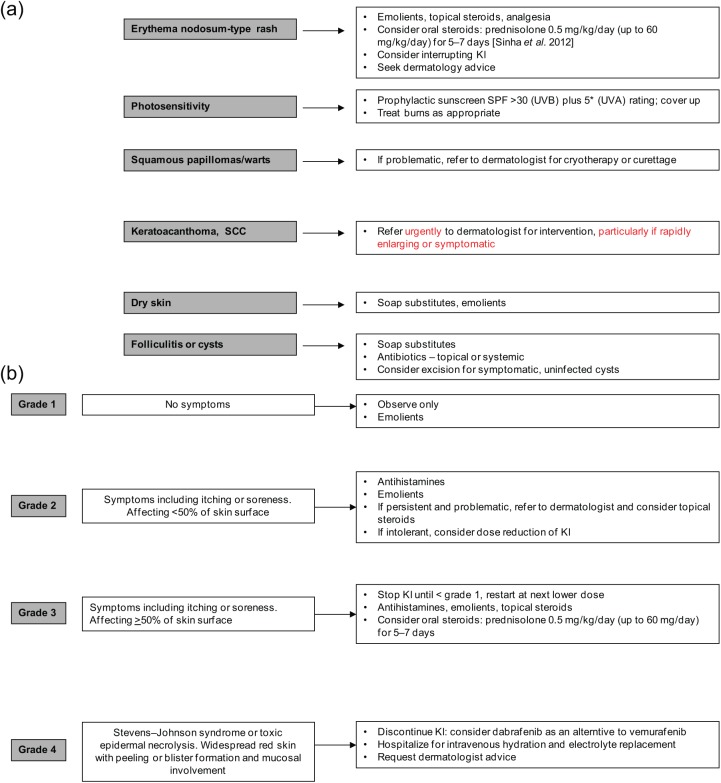
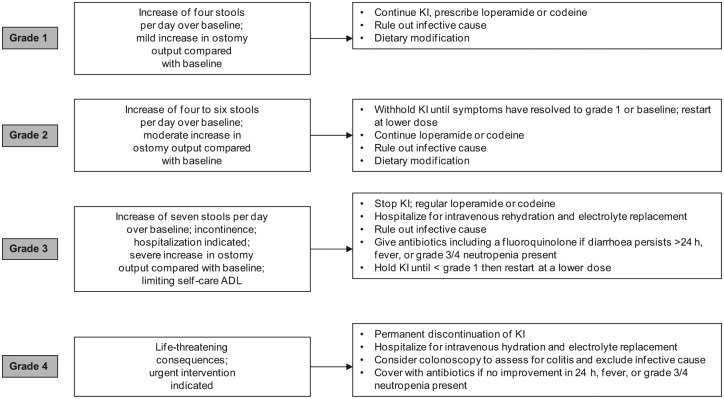
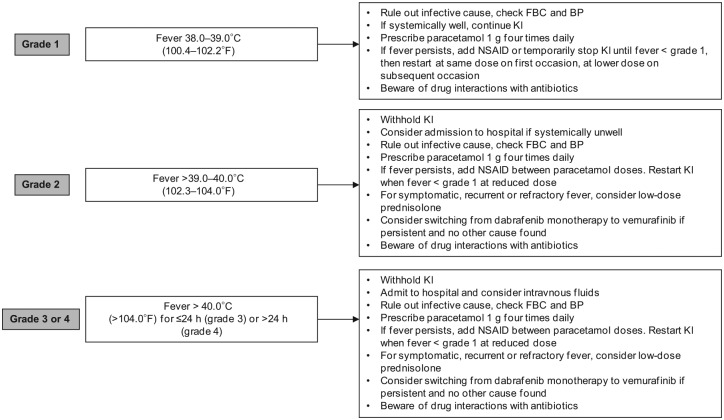
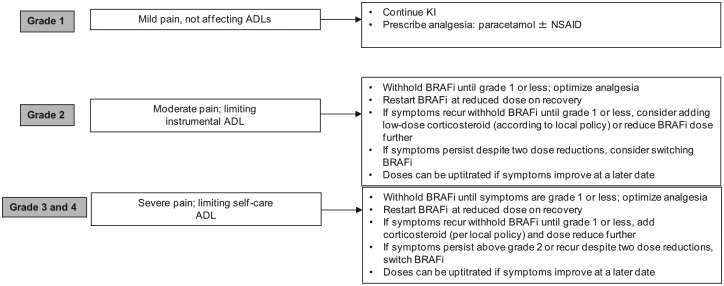
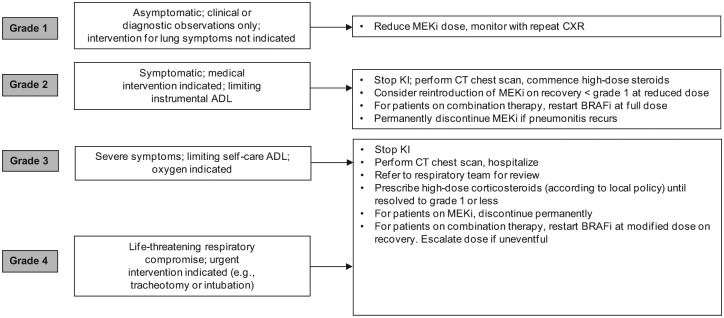
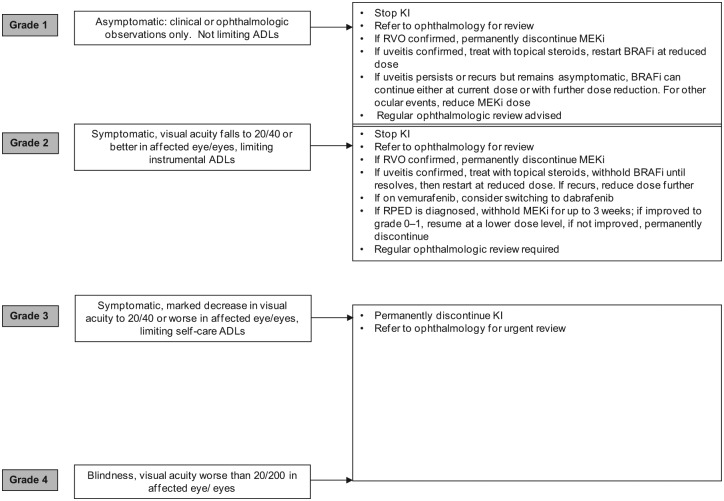
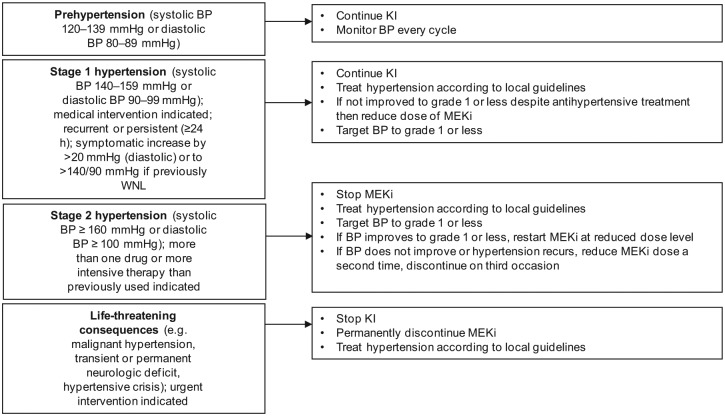
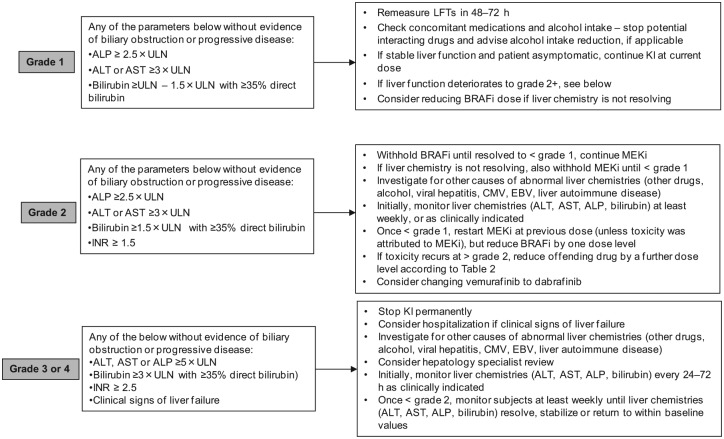
Following the discovery that nearly half of all cutaneous melanomas harbour a mutation in the BRAF gene, molecular targeted kinase inhibitors have been developed for the treatment of metastatic melanoma and have dramatically improved outcomes for those patients with BRAF mutant disease, achieving high levels of objective response and prolonging survival. Since 2011, the specific BRAF targeted agents, vemurafenib and dabrafenib, and the MEK inhibitor, trametinib, have been licensed for the treatment of patients with unresectable or metastatic BRAF mutant melanoma. As with other biological targeted agents, these drugs are associated with predictable patterns of adverse events. Proactive toxicity management is important to ensure maximum treatment benefit and avoid unnecessary treatment discontinuation. We review the most common and serious adverse events associated with BRAF targeted agents and suggest management algorithms to guide practitioners in using these drugs effectively in the clinic.
Keywords: BRAF inhibitor; MEK inhibitor; dabrafenib; management; melanoma; toxicity; trametinib; vemurafenib.
Conflict of interest statement
Figures

References
-
- Andrews M., Behren A., Chionh F., Mariadason J., Vella L., Do H., et al. (2013) BRAF inhibitor-driven tumor proliferation in a KRAS-mutated colon carcinoma is not overcome by MEK1/2 inhibition. J Clin Oncol 31: e448–e451. - PubMed
-
- Anker C., Ribas A., Grossmann A., Chen X., Narra K., Akerley W., et al. (2013) Severe liver and skin toxicity after radiation and vemurafenib in metastatic melanoma. J Clin Oncol 31: e283–e287. - PubMed
-
- Ascierto P., Minor D., Ribas A., Lebbe C., O’Hagan A., Arya N., et al. (2013) Phase II trial (BREAK-2) of the BRAFi dabrafenib (GSK2118436) in patients with metastatic melanoma. J Clin Oncol 31: 3205–3211. - PubMed
-
- Babacan T., Türkbeyler I., Balakan O., Pehlivan Y., Suner A., Kısacık B. (2014) A case of vemurafenib-induced polyarthritis in a patient with melanoma: how to manage it? Int J Rheum Dis 12 May [Epub ahead of print]. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
