

Impact of ischemic preconditioning on outcome in clinical liver surgery: a systematic review
- PMID: 25756045
- PMCID: PMC4338382
- DOI: 10.1155/2015/370451
Impact of ischemic preconditioning on outcome in clinical liver surgery: a systematic review
Abstract
Background: Ischemia-reperfusion injury is a major cause of post-liver-surgery complications. Ischemic preconditioning (IPC) has been demonstrated to protect against ischemia-reperfusion injury. Clinical studies have examined IPC in liver surgery but with conflicting results. This systematic review aimed to evaluate the effects of IPC on outcome in clinical liver surgery.
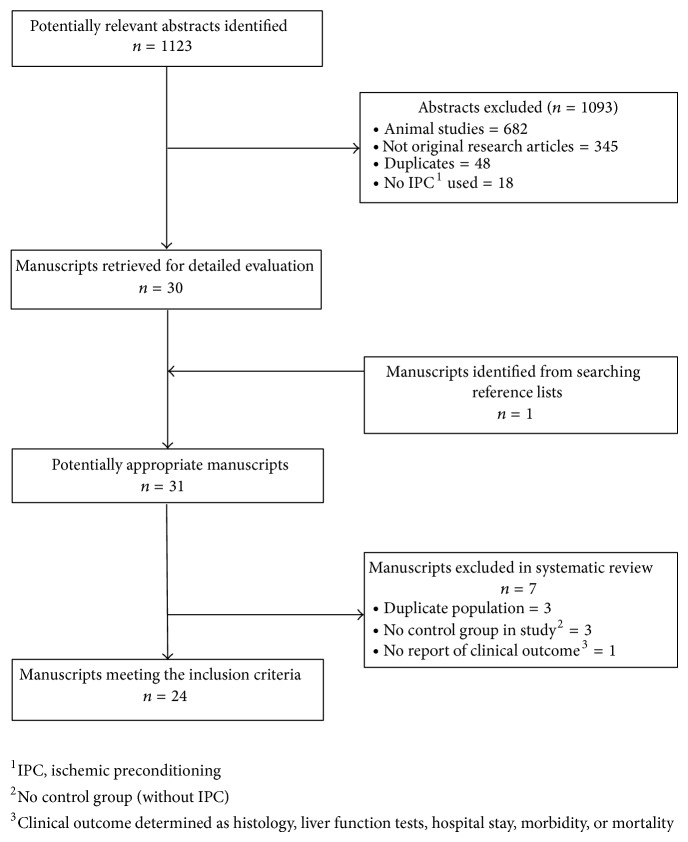
Methods: An electronic search of OVID Medline and Embase databases was performed to identify studies that reported outcomes in patients undergoing liver surgery subjected to IPC. Basic descriptive statistics were used to summarise data from individual clinical studies.
Results: 1093 articles were identified, of which 24 met the inclusion criteria. Seven topics were selected and analysed by subgroup. There were 10 studies in cadaveric liver transplantation, 2 in living-related liver transplantation, and 12 in liver resection. IPC decreases hepatocellular damage in liver surgery as determined by transaminases but does not translate to any significant clinical benefit in orthotopic liver transplant or liver resection.
Conclusions: Available clinical evidence does not support routine use of IPC in liver surgery as it does not offer any apparent benefit in perioperative outcome. Further clinical studies will need to be carried out to determine the subset of patients that will benefit from IPC.
References
-
- Veteläinen R., van Vliet A., Gouma D. J., van Gulik T. M. Steatosis as a risk factor in liver surgery. Annals of Surgery. 2007;245(1):20–30. doi: 10.1097/01.sla.0000225113.88433.cf. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
