

Enhanced perfusion during advanced life support improves survival with favorable neurologic function in a porcine model of refractory cardiac arrest
- PMID: 25756411
- PMCID: PMC4860001
- DOI: 10.1097/CCM.0000000000000939
Enhanced perfusion during advanced life support improves survival with favorable neurologic function in a porcine model of refractory cardiac arrest
Abstract
Objective: To improve the likelihood for survival with favorable neurologic function after cardiac arrest, we assessed a new advanced life support approach using active compression-decompression cardiopulmonary resuscitation plus an intrathoracic pressure regulator.
Design: Prospective animal investigation.
Setting: Animal laboratory.
Subjects: Female farm pigs (n = 25) (39 ± 3 kg).
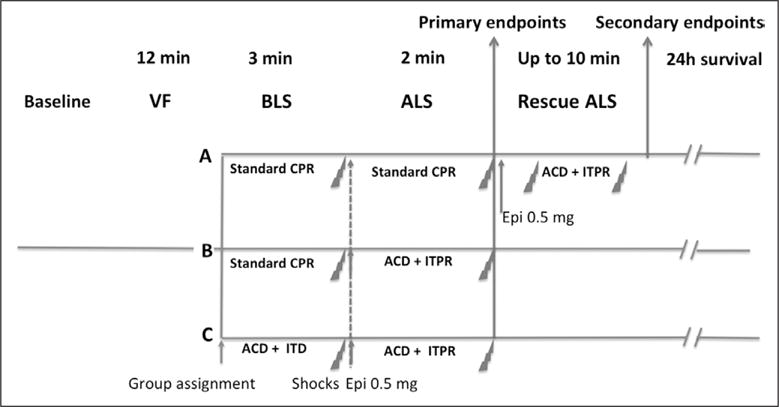
Interventions: Protocol A: After 12 minutes of untreated ventricular fibrillation, 18 pigs were randomized to group A-3 minutes of basic life support with standard cardiopulmonary resuscitation, defibrillation, and if needed 2 minutes of advanced life support with standard cardiopulmonary resuscitation; group B-3 minutes of basic life support with standard cardiopulmonary resuscitation, defibrillation, and if needed 2 minutes of advanced life support with active compression-decompression plus intrathoracic pressure regulator; and group C-3 minutes of basic life support with active compression-decompression cardiopulmonary resuscitation plus an impedance threshold device, defibrillation, and if needed 2 minutes of advanced life support with active compression-decompression plus intrathoracic pressure regulator. Advanced life support always included IV epinephrine (0.05 μg/kg). The primary endpoint was the 24-hour Cerebral Performance Category score. Protocol B: Myocardial and cerebral blood flow were measured in seven pigs before ventricular fibrillation and then following 6 minutes of untreated ventricular fibrillation during sequential 5 minutes treatments with active compression-decompression plus impedance threshold device, active compression-decompression plus intrathoracic pressure regulator, and active compression-decompression plus intrathoracic pressure regulator plus epinephrine.
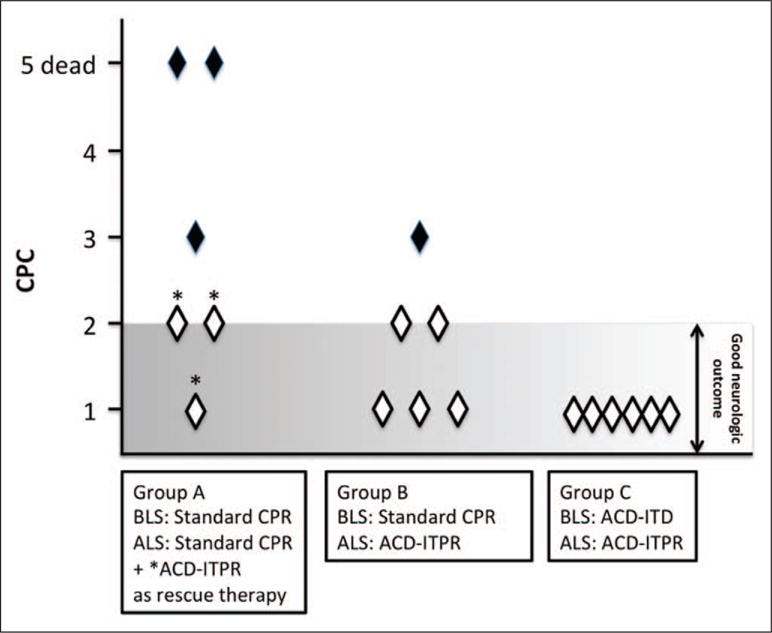
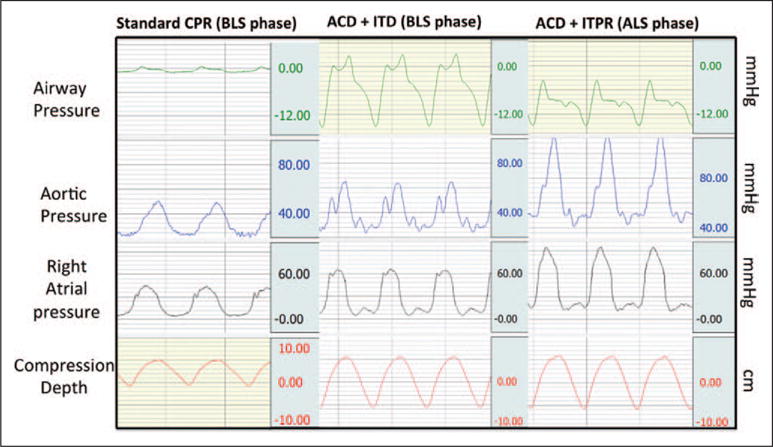
Measurements and main results: Protocol A: One of six pigs survived for 24 hours in group A versus six of six in groups B and C (p = 0.002) and Cerebral Performance Category scores were 4.7 ± 0.8, 1.7 ± 0.8, and 1.0 ± 0, respectively (p = 0.001). Protocol B: Brain blood flow was significantly higher with active compression-decompression plus intrathoracic pressure regulator compared with active compression-decompression plus impedance threshold device (0.39 ± 0.23 vs 0.27 ± 0.14 mL/min/g; p = 0.03), whereas differences in myocardial perfusion were not statistically significant (0.65 ± 0.81 vs 0.42 ± 0.36 mL/min/g; p = 0.23). Brain and myocardial blood flow with active compression-decompression plus intrathoracic pressure regulator plus epinephrine were significantly increased versus active compression-decompression plus impedance threshold device (0.40 ± 0.22 and 0.84 ± 0.60 mL/min/g; p = 0.02 for both).
Conclusion: Advanced life support with active compression-decompression plus intrathoracic pressure regulator significantly improved cerebral perfusion and 24-hour survival with favorable neurologic function. These findings support further evaluation of this new advanced life support methodology in humans.
Figures
Similar articles
-
Improved cerebral perfusion pressures and 24-hr neurological survival in a porcine model of cardiac arrest with active compression-decompression cardiopulmonary resuscitation and augmentation of negative intrathoracic pressure.Crit Care Med. 2012 Jun;40(6):1851-6. doi: 10.1097/CCM.0b013e318246b9ad. Crit Care Med. 2012. PMID: 22487997 Free PMC article.
-
Reperfusion injury protection during Basic Life Support improves circulation and survival outcomes in a porcine model of prolonged cardiac arrest.Resuscitation. 2016 Aug;105:29-35. doi: 10.1016/j.resuscitation.2016.05.008. Epub 2016 May 20. Resuscitation. 2016. PMID: 27211835
-
Sodium nitroprusside-enhanced cardiopulmonary resuscitation facilitates intra-arrest therapeutic hypothermia in a porcine model of prolonged ventricular fibrillation.Crit Care Med. 2015 Apr;43(4):849-55. doi: 10.1097/CCM.0000000000000825. Crit Care Med. 2015. PMID: 25525755 Free PMC article.
-
Combination of active compression decompression cardiopulmonary resuscitation and the inspiratory impedance threshold device: state of the art.Curr Opin Crit Care. 2004 Jun;10(3):193-201. doi: 10.1097/01.ccx.0000126089.40242.a9. Curr Opin Crit Care. 2004. PMID: 15166836 Review.
-
Vital organ blood flow with the impedance threshold device.Crit Care Med. 2006 Dec;34(12 Suppl):S466-73. doi: 10.1097/01.CCM.0000246013.47237.86. Crit Care Med. 2006. PMID: 17114979 Review.
Cited by
-
Dynamic cerebral autoregulation is preserved during orthostasis and intrathoracic pressure regulation in healthy subjects: A pilot study.Physiol Rep. 2024 May;12(9):e16027. doi: 10.14814/phy2.16027. Physiol Rep. 2024. PMID: 38684421 Free PMC article.
-
Sodium nitroprusside enhanced cardiopulmonary resuscitation improves short term survival in a porcine model of ischemic refractory ventricular fibrillation.Resuscitation. 2017 Jan;110:6-11. doi: 10.1016/j.resuscitation.2016.09.032. Epub 2016 Oct 19. Resuscitation. 2017. PMID: 27771299 Free PMC article.
-
Effects of mechanical ventilation with expiratory negative airway pressure on porcine pulmonary and systemic circulation: mechano-physiology and potential application.J Physiol Sci. 2021 Jun 2;71(1):17. doi: 10.1186/s12576-021-00801-5. J Physiol Sci. 2021. PMID: 34078262 Free PMC article.
-
Personalized physiology-guided resuscitation in highly monitored patients with cardiac arrest-the PERSEUS resuscitation protocol.Heart Fail Rev. 2019 Jul;24(4):473-480. doi: 10.1007/s10741-019-09772-7. Heart Fail Rev. 2019. PMID: 30741366 Review.
-
Left rib fractures during cardiopulmonary resuscitation are associated with hemodynamic variations in a pig model of cardiac arrest.Resusc Plus. 2023 Jul 14;15:100429. doi: 10.1016/j.resplu.2023.100429. eCollection 2023 Sep. Resusc Plus. 2023. PMID: 37502743 Free PMC article.
References
-
- Cohen TJ, Tucker KJ, Lurie KG, et al. Active compression-decompression. A new method of cardiopulmonary resuscitation Cardiopulmonary Resuscitation Working Group. JAMA. 1992;267:2916–2923. - PubMed
-
- Lurie KG, Lindner KH. Recent advances in cardiopulmonary resuscitation. J Cardiovasc Electrophysiol. 1997;8:584–600. - PubMed
-
- Duggal C, Weil MH, Gazmuri RJ, et al. Regional blood flow during closed-chest cardiac resuscitation in rats. J Appl Physiol (1985) 1993;74:147–152. - PubMed
-
- Olasveengen TM, Sunde K, Brunborg C, et al. Intravenous drug administration during out-of-hospital cardiac arrest: A randomized trial. JAMA. 2009;302:2222–2229. - PubMed
-
- Stiell IG, Wells GA, Field B, et al. Ontario Prehospital Advanced Life Support Study Group Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351:647–656. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
