

Increased visceral adipose tissue as a potential risk factor in patients with embolic stroke of undetermined source (ESUS)
- PMID: 25756793
- PMCID: PMC4354901
- DOI: 10.1371/journal.pone.0120598
Increased visceral adipose tissue as a potential risk factor in patients with embolic stroke of undetermined source (ESUS)
Abstract
Purpose: The etiology of an ischemic stroke remains undetermined in 20-35% of cases and many patients do not have any of the conventional risk factors. Increased visceral adipose tissue (VAT) is a suggested new risk factor for both carotid artery atherosclerosis (CAA) and atrial fibrillation (AF), but its role in the remaining stroke population is unknown. We assessed the amount of VAT in patients with embolic stroke of undetermined source (ESUS) after excluding major-risk cardioembolic sources, occlusive atherosclerosis, and lacunar stroke.
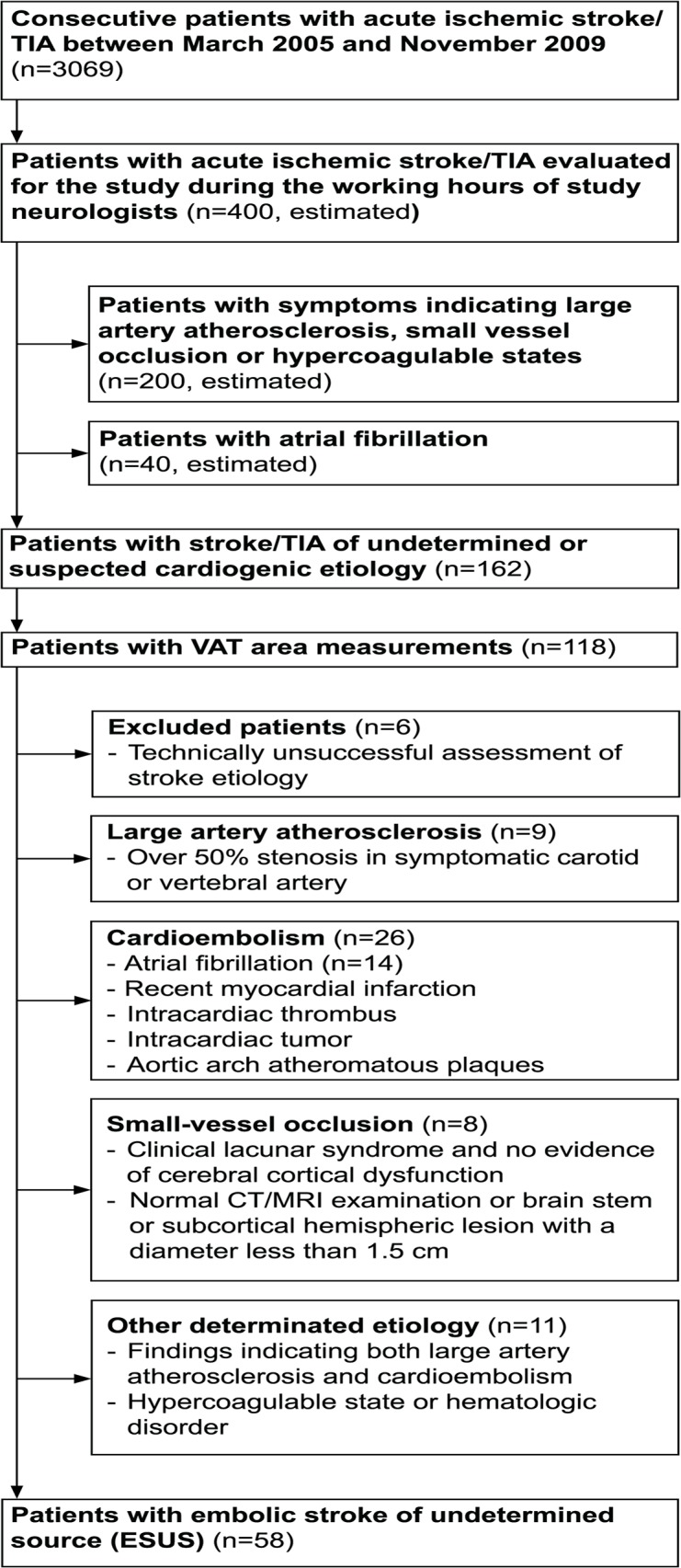
Methods: Altogether 58 patients (mean age 57.7 ± 10.2 years, 44 men) with ischemic stroke of unknown etiology but without CAA, known AF or small vessel disease underwent computed tomography angiography and assessment of VAT. For comparison VAT values from three different reference populations were used. Conventional risk factors (smoking, hypertension, diabetes, increased total and LDL-cholesterol, decreased HDL-cholesterol) were also registered.
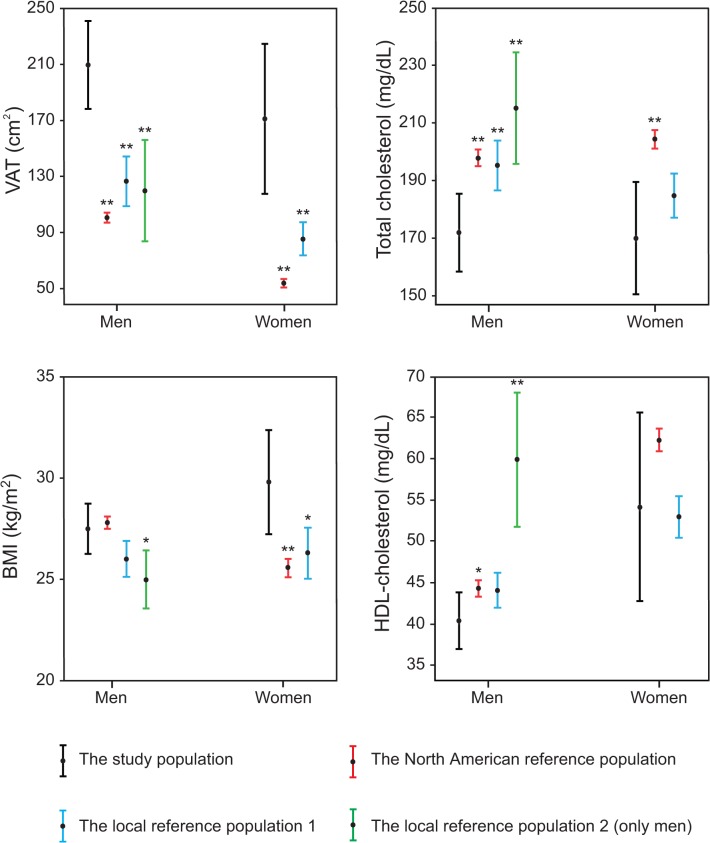
Results: Mean VAT area was significantly higher in stroke patients (205 ± 103 cm2 for men and 168 ± 99 cm2 for women) compared to all reference populations (P < 0.01). 50% of male and 57% of female patients had an increased VAT area. In male patients, VAT was significantly higher despite similar body mass index (BMI). Increased VAT was more common than any of the conventional risk factors.
Conclusion: Increased VAT was found in over half of our patients with ESUS suggesting it may have a role in the pathogenesis of thromboembolism in this selected group of patients.
Conflict of interest statement
Figures

References
-
- Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet 2006;367: 1747–1757. - PubMed
-
- Sacco RL, Adams R, Albers G, Alberts MJ, Benavente O, Furie K, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack. Stroke 2006;37: 577–617. - PubMed
-
- World Health Organization. World health statistics 2012 Geneva, Switzerland: World health organization; 2012.
-
- Ay H, Furie KL, Singhal A, Smith WS, Sorensen AG, Koroshetz WJ. An evidence-based causative classification system for acute ischemic stroke. Ann Neurol 2005;58: 688–697. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
