

A Reassessment of the Survival Advantage of Simultaneous Kidney-Pancreas Versus Kidney-Alone Transplantation
- PMID: 25757212
- PMCID: PMC4548542
- DOI: 10.1097/TP.0000000000000663
A Reassessment of the Survival Advantage of Simultaneous Kidney-Pancreas Versus Kidney-Alone Transplantation
Abstract
Background: Simultaneous kidney and pancreas (SPK) transplantation is an attractive option for end-stage renal disease patients with type 1 diabetes. Although SPK transplantation is superior to remaining on dialysis, the survival advantage for SPK recipients compared to kidney transplantation alone (KTA) is controversial.
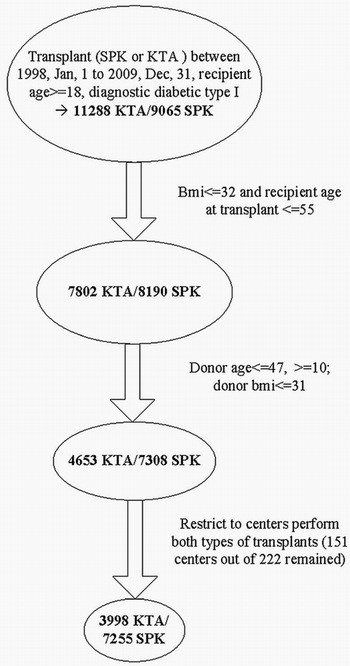
Methods: Using data obtained from the Scientific Registry of Transplant Recipients, we compared patient and graft survivals for 7308 SPK and 4653 KTA adult patients with type I diabetes transplanted in 1998 to 2009. Because SPK and KTA recipients are differently selected, comparison groups were chosen to maximize overlap in the case mixes. Most previous studies contrasted (unadjusted) Kaplan-Meier survival curves or, if covariate-adjusted, reported hazard ratios (HRs). Using newer statistical methods, we avoid relying on hazard ratios (which are seldom of inherent interest) and directly compare covariate-adjusted survival curves. Specifically, we compare average covariate-adjusted SPK- and KTA-specific survival curves (and 10-year area under the curve; ie, restricted mean survival time) to emulate a randomized clinical trial.
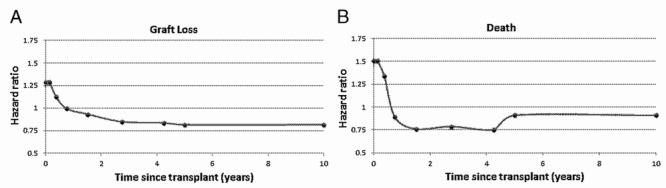
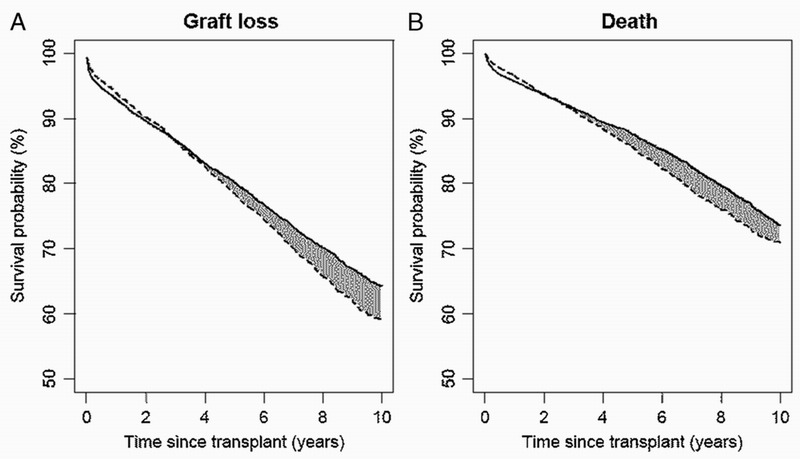
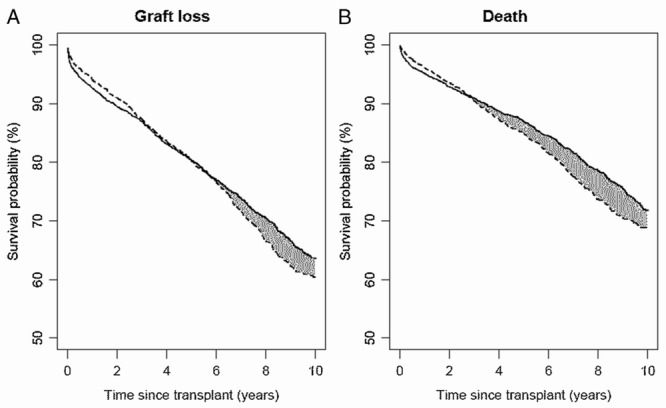
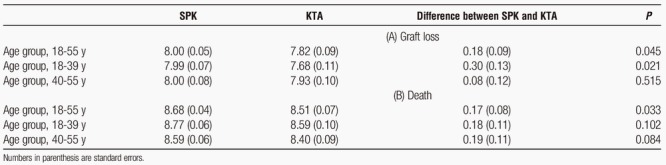
Results: Mean restricted mean kidney graft survival time was significantly greater by 0.18 years (P = 0.045) for SPK compared to KTA. Similarly, patient survival was 0.17 years greater (P = 0.033) for SPK than KTA. Increased graft survival was primarily observed in younger SPK recipients. Supplementary analysis revealed that the SPK hazards were nonproportional, meaning that it would be difficult to quantify the cumulative effect of SPK through a standard Cox regression analysis.
Conclusions: Using this novel methodology, we demonstrate that SPK is associated with statistically but not clinically significant increases in graft and patient survival.
Figures
Comment in
-
Response to A reassessment of the Survival Advantage of Simultaneous Kidney-Pancreas Versus Kidney-Alone Transplantation.Transplantation. 2015 Nov;99(11):e175. doi: 10.1097/TP.0000000000000839. Transplantation. 2015. PMID: 26492056 No abstract available.
References
-
- Kalbfleisch JD, Prentice RL. The Statistical Analysis of Failure Time Data. New York: Wiley; 2002.
-
- Rao PS, Schaubel DE, Guidinger MK, et al. A comprehensive risk quantification score for deceased donor kidneys: the Kidney Donor Risk Index. Transplantation. 2009; 88: 231– 236. - PubMed
-
- Chen P, Tsiatis AA. Causal inference on the difference of the restricted mean life between two groups. Biometrics. 2001; 57: 1030– 1038. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
