

Cafedrine/theodrenaline in anaesthesia: influencing factors in restoring arterial blood pressure
- PMID: 25757552
- PMCID: PMC4383809
- DOI: 10.1007/s00101-015-0005-y
Cafedrine/theodrenaline in anaesthesia: influencing factors in restoring arterial blood pressure
Abstract
Background: Hypotensive states that require fast stabilisation of blood pressure can occur during anaesthesia. In 1963, the 20:1 mixture of cafedrine/theodrenaline (Akrinor) was introduced in Germany for use in anaesthesia and emergency medicine in the first-line management of hypotensive states. Though on the market for many years, few pharmacodynamic data are available on this combination net beta-mimetic agent.
Aim: This study aimed to examine the drug combination in real-life clinical practice and recorded time to 10 % mean arterial blood pressure (MAP) increase and heart rate. Furthermore, potential factors that influence drug effectiveness under anaesthesia were assessed.
Methods: Data were collected within a standardised anaesthesia protocol. A total of 353 consecutive patients (female/male = 149/204) who received cafedrine/theodrenaline after a drop in MAP ≥ 5% were included in the study. The time to 10 % increase in MAP, dosage of cafedrine/theodrenaline, volume loading, blood pressure and heart rate were monitored over time.
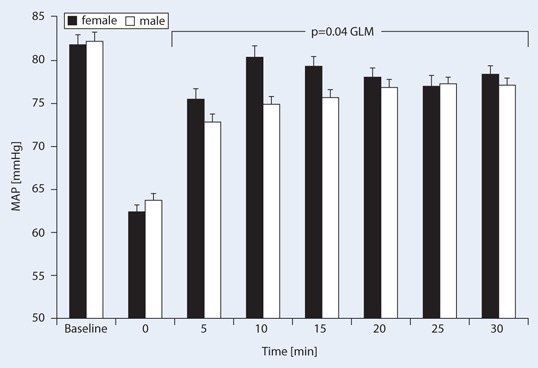
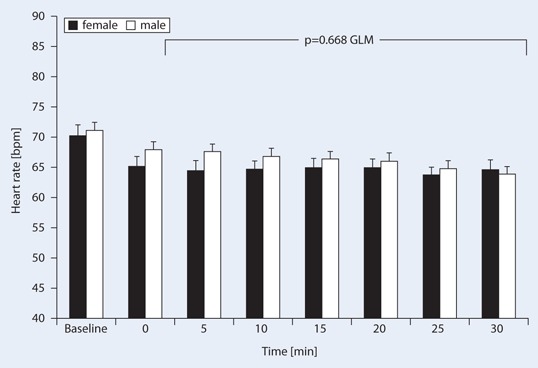
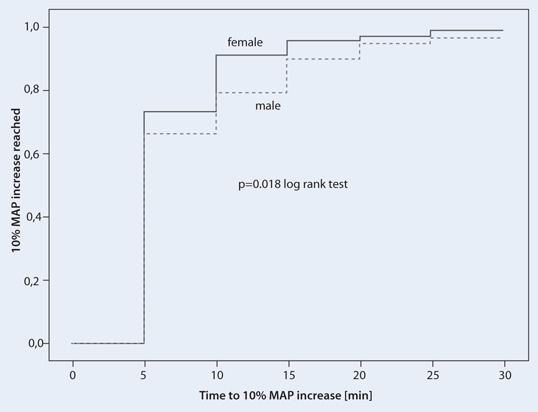
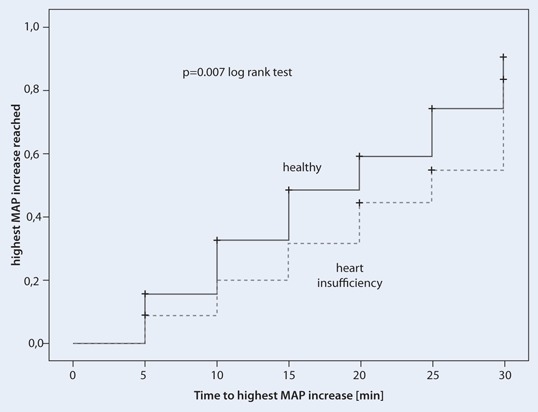
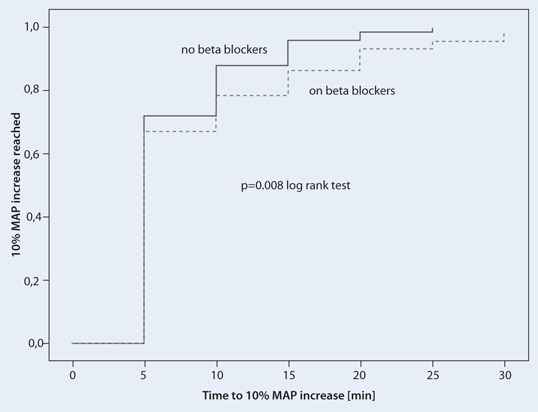
Results: Patients were a mean (standard deviation) of 64.4 ± 15.1 years old with a baseline MAP of 82 ± 14 mmHg, which dropped to a mean of 63 ± 10 mmHg during anaesthesia without gender differences. Cafedrine/theodrenaline (1.27 ± 1.0 mg/kg; 64 ± 50 µg/kg) significantly increased MAP (p < 0.001) by 11 ± 16 mmHg within 5 min, reaching peak values within 17.4 ± 9.0 min. Heart rate was not affected in a clinically significant manner. Cafedrine/theodrenaline induced a 10% MAP increase after 7.2 ± 4.6 min (women) and after 8.6 ± 6.3 min (men) (p = 0.018). Independent of gender, the dose of cafedrine/theodrenaline required to achieve the observed MAP increase of 14 ± 16 mmHg at 15 min was significantly different in patients with heart failure [1.78 ± 1.67 mg/kg (cafedrine)/89.0 ± 83.5 µg/kg (theodrenaline)] compared with healthy patients [1.16 ± 0.77 mg/kg (cafedrine)/58.0 ± 38.5 µg/kg (theodrenaline)] (p = 0.005). Concomitant medication with beta-blocking agents significantly prolonged the time to 10 % MAP increase [9.0 ± 7.0 vs. 7.3 ± 4.3 min (p = 0.008)].
Conclusion: Cafedrine/theodrenaline quickly restores MAP during anaesthesia. Female gender is associated with higher effectiveness, while heart failure and beta-blocker administration lower the anti-hypotonic effect. Prospective studies in defined patient populations are warranted to further characterise the effect of cafedrine/theodrenaline.
Hintergrund: Cafedrin/Theodrenalin (Akrinor®) wird in Deutschland für die Therapie von Blutdruckabfällen in Anästhesie und Notfallmedizin verwendet.
Ziel der Arbeit (Fragestellung): Die Studie untersucht potentielle Faktoren, die die Wirksamkeit des Arzneimittels beeinflussen.
Material und Methoden: Patientendaten wurden mittels Anästhesie-Protokollen gesammelt. 353 Patienten (weiblich/männlich = 149/204), die Cafedrin/Theodrenalin nach einem Abfall des mittleren arteriellen Blutdrucks (MAP) ≥ 5 % erhielten, wurden einbezogen.
Ergebnisse: Die Patienten waren 64,4 ± 15,1 Jahre alt und hatten einen Ausgangs-MAP von 82 ± 14 mmHg, der während der Anästhesie unabhängig von Geschlecht auf einen Mittelwert von 63 ± 10 mmHg abfiel.
Cafedrin/Theodrenalin (1,27 ± 1,0 mg/kg/64 ± 50 µg/kg) erhöhte den MAP innerhalb von 5 min um 11 ± 16 mmHg (p < 0,001). Der maximale MAP war nach 17,4 ± 9,0 min erreicht; die Herzfrequenz wurde nicht im klinisch signifikanten Maß verändert. Cafedrin/Theodrenalin induzierte einen 10 % MAP-Anstieg nach 7,2 ± 4,6 min bei Frauen und nach 8,6 ± 6,3 min bei Männern (p = 0,018). Unabhängig vom Geschlecht waren die Dosen von Cafedrin/Theodrenalin, die zu dem beobachteten MAP-Anstieg um 14 ± 16 mmHg nach 15 min führten, signifikant unterschiedlich zwischen Patienten mit und ohne Herzinsuffizienz (1,78 ± 1,67 mg/kg (Cafedrin)/89,0 ± 83,5 µg/kg (Theodrenalin) vs. 1,16 ± 0,77 mg/kg (Cafedrin)/58,0 ± 38,5 µg/kg (Theodrenalin), p = 0,005).
Gleichzeitige Medikation mit Betablockern verlängerte die Zeit bis zum 10 % MAP-Anstieg [9,0 ± 7,0 vs. 7,3 ± 4,3 min (p = 0,008)].
Schlussfolgerung: Theodrenalin/Cafedrin stellt den MAP nach Blutdruckabfällen schnell wieder her ohne die Herzfrequenz klinisch relevant zu verändern. Das Medikament zeigt eine höhere Wirksamkeit bei Frauen, während Herzinsuffizienz und Betablocker den Effekt schwächen.
Conflict of interest statement
Julia Heger, Marcelo Gama de Abreu, Michael P. Müller declare no conflict of interest.
Figures
References
-
- Brandstrup B, Tonnesen H, Beier-Holgersen R, Hjortso E, Ording H, Lindorff-Larsen K, Rasmussen MS, Lanng C, Wallin L, Iversen LH, Gramkow CS, Okholm M, Blemmer T, Svendsen PE, Rottensten HH, Thage B, Riis J, Jeppesen IS, Teilum D, Christensen AM, Graungaard B, Pott F. Effects of intravenous fluid restriction on postoperative complications: comparison of two perioperative fluid regimens: a randomized assessor-blinded multicenter trial. Ann Surg. 2003;238:641–648. doi: 10.1097/01.sla.0000094387.50865.23. - DOI - PMC - PubMed
-
- Carl M, Alms A, Braun J, Dongas A, Erb J, Goetz A, Gopfert M, Gogarten W, Grosse J, Heller A, Heringlake M, Kastrup M, Kroner A, Loer S, Marggraf G, Markewitz A, Reuter M, Schmitt DV, Schirmer U, Wiesenack C, Zwissler B, Spies C. Guidelines for intensive care in cardiac surgery patients: haemodynamic monitoring and cardio-circulatory treatment guidelines of the German Society for Thoracic and Cardiovascular Surgery and the German Society of anaesthesiology and intensive care medicine. Thorac Cardiovasc Surg. 2007;55:130–148. doi: 10.1055/s-2007-964939. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
