

Abnormal White Matter Blood-Oxygen-Level-Dependent Signals in Chronic Mild Traumatic Brain Injury
- PMID: 25758167
- PMCID: PMC4601555
- DOI: 10.1089/neu.2014.3547
Abnormal White Matter Blood-Oxygen-Level-Dependent Signals in Chronic Mild Traumatic Brain Injury
Abstract
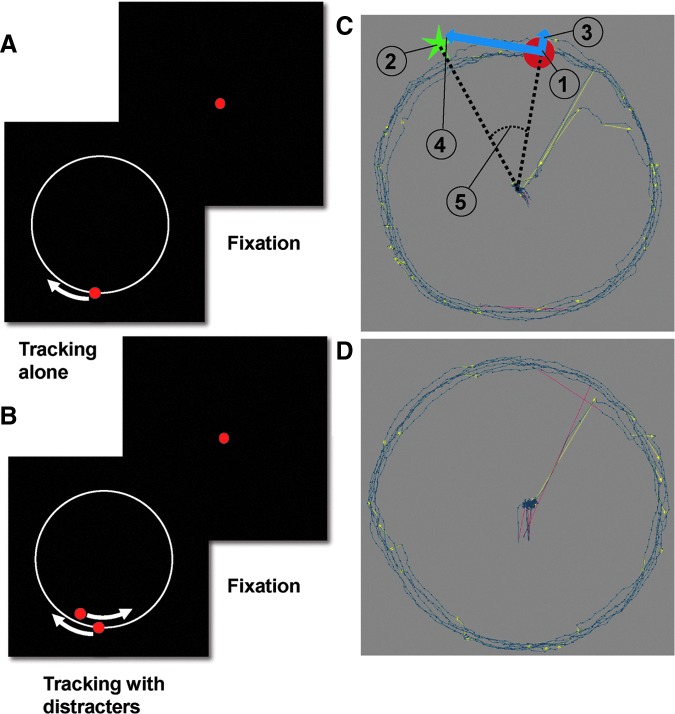
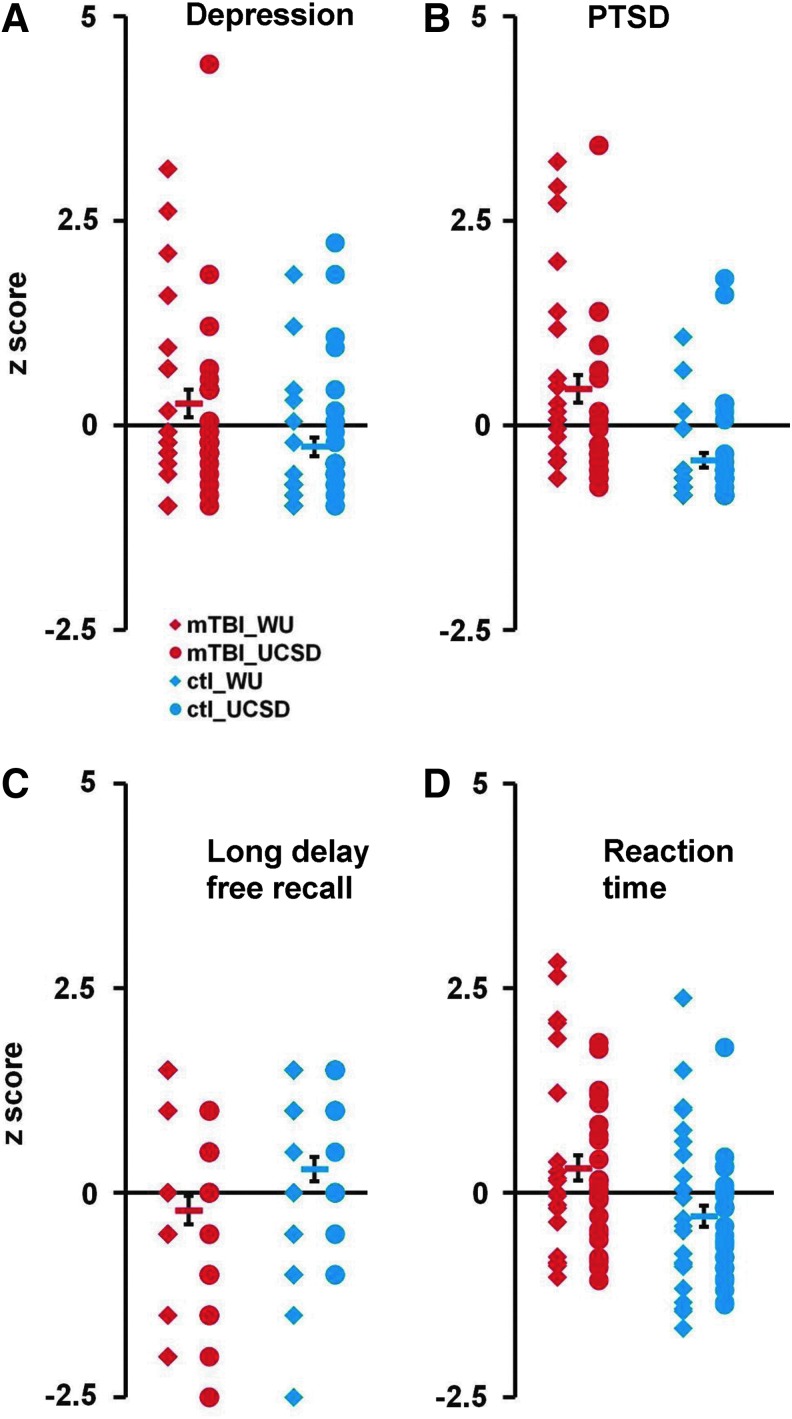
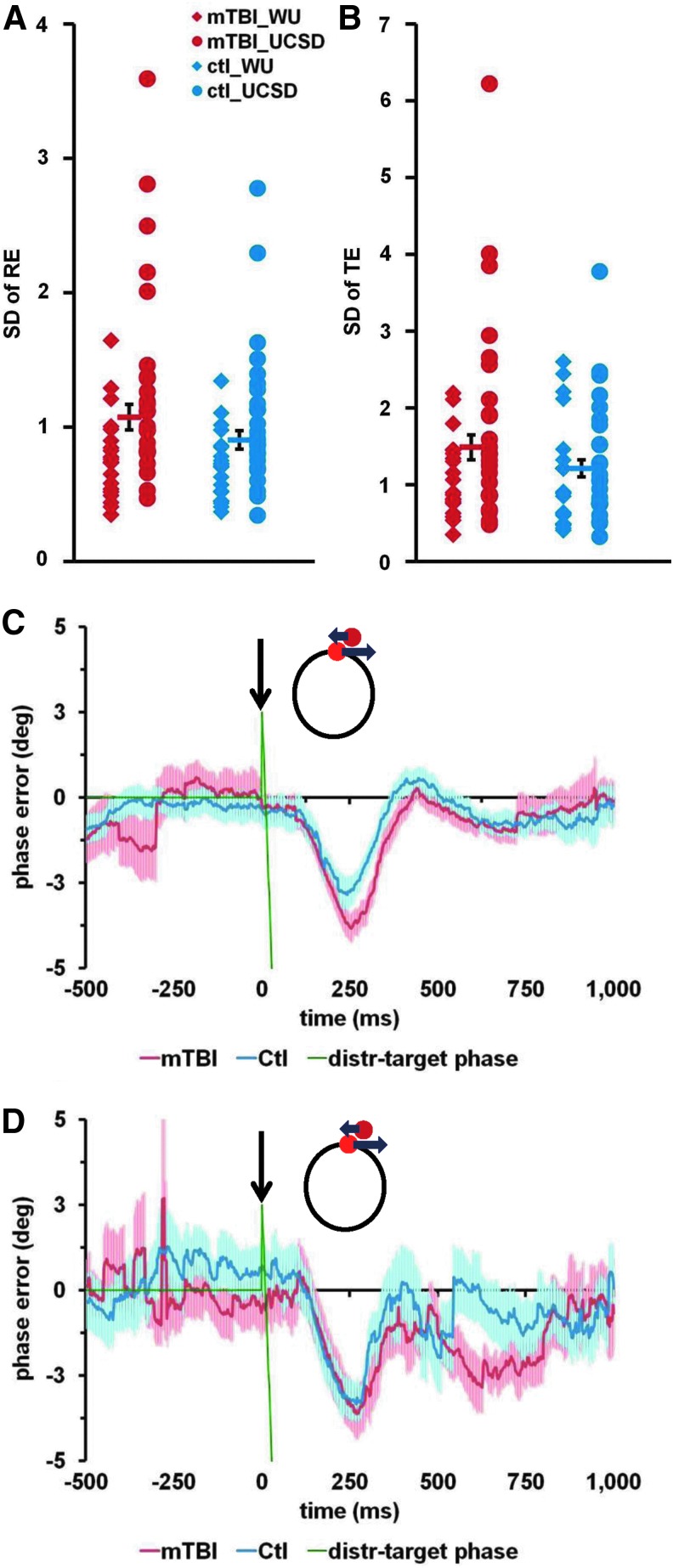
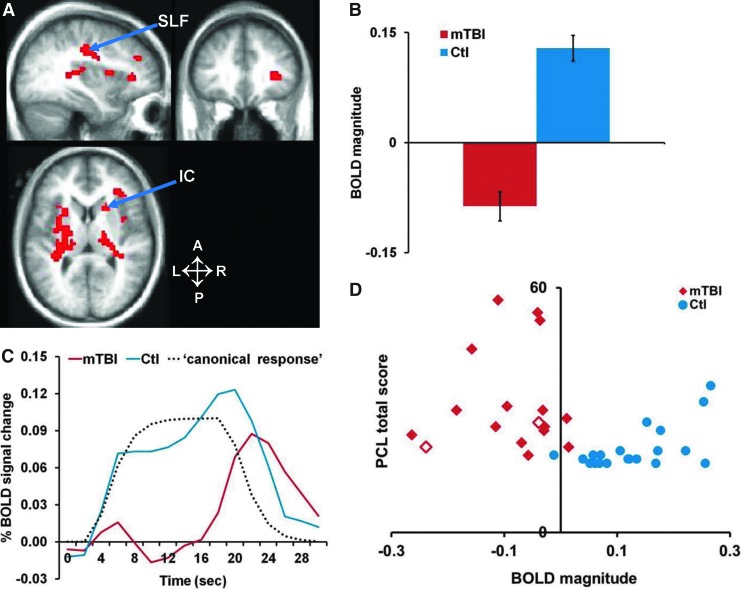
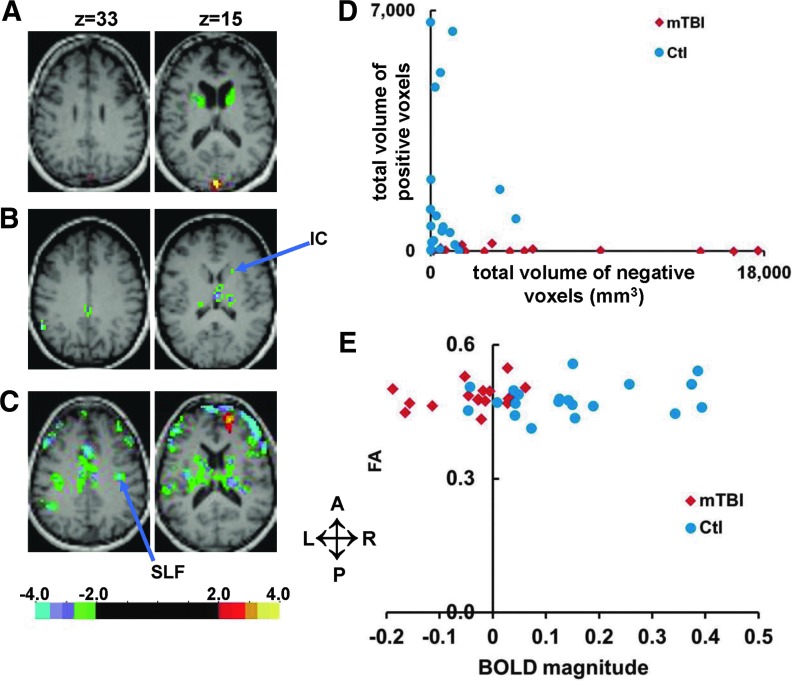
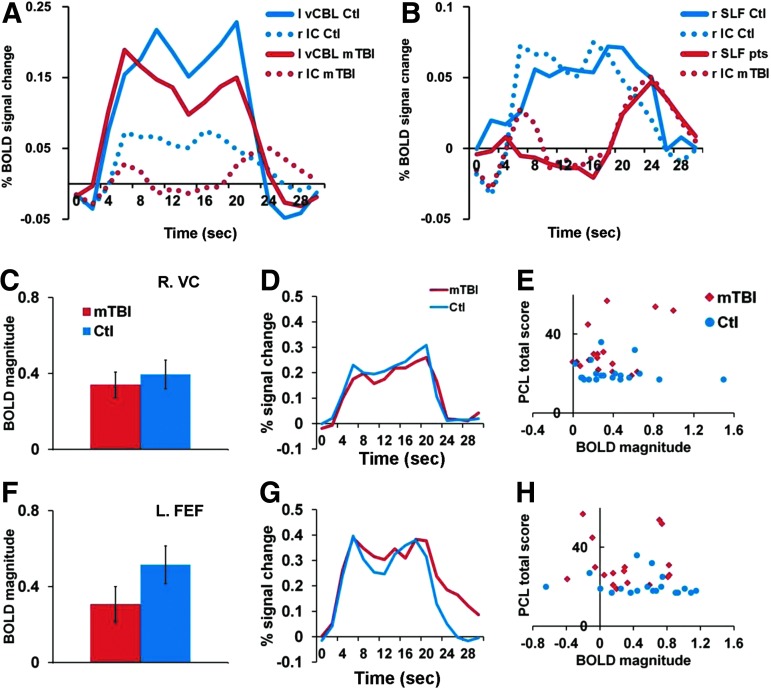
Concussion, or mild traumatic brain injury (mTBI), can cause persistent behavioral symptoms and cognitive impairment, but it is unclear if this condition is associated with detectable structural or functional brain changes. At two sites, chronic mTBI human subjects with persistent post-concussive symptoms (three months to five years after injury) and age- and education-matched healthy human control subjects underwent extensive neuropsychological and visual tracking eye movement tests. At one site, patients and controls also performed the visual tracking tasks while blood-oxygen-level-dependent (BOLD) signals were measured with functional magnetic resonance imaging. Although neither neuropsychological nor visual tracking measures distinguished patients from controls at the level of individual subjects, abnormal BOLD signals were reliably detected in patients. The most consistent changes were localized in white matter regions: anterior internal capsule and superior longitudinal fasciculus. In contrast, BOLD signals were normal in cortical regions, such as the frontal eye field and intraparietal sulcus, that mediate oculomotor and attention functions necessary for visual tracking. The abnormal BOLD signals accurately differentiated chronic mTBI patients from healthy controls at the single-subject level, although they did not correlate with symptoms or neuropsychological performance. We conclude that subjects with persistent post-concussive symptoms can be identified years after their TBI using fMRI and an eye movement task despite showing normal structural MRI and DTI.
Keywords: MRI; behavioral assessments; diffusion tensor imaging; traumatic brain injury.
Figures

References
-
- Coronado V.G., McGuire L.C., Faul M., Sugerman D., and Pearson W. (2012). The Epidemiology and Prevention of TBI (in press)
-
- Narayan R.K., Michel M.E., Ansell B., Baethmann A., Biegon A., Bracken M.B., Bullock M.R., Choi S.C., Clifton G.L., Contant C.F., Coplin W.M., Dietrich W.D., Ghajar J., Grady S.M., Grossman R.G., Hall E.D., Heetderks W., Hovda D.A., Jallo J., Katz R.L., Knoller N., Kochanek P.M., Maas A.I., Majde J., Marion D.W., Marmarou A., Marshall L.F., McIntosh T.K., Miller E., Mohberg N., Muizelaar J.P., Pitts L.H., Quinn P., Riesenfeld G., Robertson C.S., Strauss K.I., Teasdale G., Temkin N., Tuma R., Wade C., Walker M.D., Weinrich M., Whyte J., Wilberger J., Young A.B., and Yurkewicz L. (2002). Clinical trials in head injury. J. Neurotrauma 19, 503–557 - PMC - PubMed
-
- Ghajar J. (2000). Traumatic brain injury. Lancet 356, 923–929 - PubMed
-
- Kushner D. (1998). Mild traumatic brain injury: toward understanding manifestations and treatment. Arch. Intern. Med. 158, 1617–1624 - PubMed
-
- Gerber D.J. and Schraa J.C. (1995). Mild traumatic brain injury: searching for the syndrome. J. Head Trauma Rehabil. 10, 28–40
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
