

Contemporary management of median arcuate ligament syndrome provides early symptom improvement
- PMID: 25758451
- PMCID: PMC5292272
- DOI: 10.1016/j.jvs.2015.01.050
Contemporary management of median arcuate ligament syndrome provides early symptom improvement
Abstract
Objective: Optimal diagnosis and management of median arcuate ligament (MAL) syndrome (MALS) remains unclear in contemporary practice. The advent and evolution of laparoscopic and endovascular techniques has redirected management toward a less invasive therapeutic algorithm. This study examined our contemporary outcomes of patients treated for MALS.
Methods: All patients treated for MALS at Dartmouth-Hitchcock Medical Center from 2000 to 2013 were retrospectively reviewed. Demographics and comorbidities were recorded. Freedom from symptoms and freedom from reintervention were the primary end points. Return to work or school was assessed. Follow-up by clinic visits and telephone allowed quantitative comparisons among the patients.
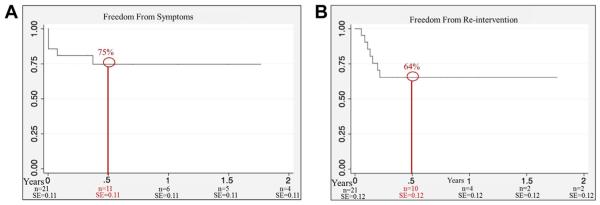
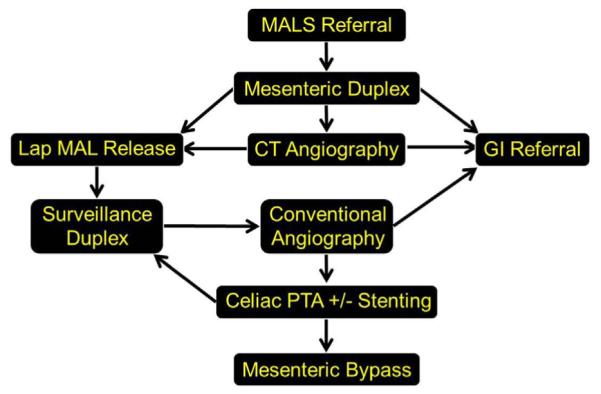
Results: During the study interval, 21 patients (24% male), with a median age of 42 years, were treated for MALS. All patients complained of abdominal pain in the presence of a celiac stenosis, 16 (76%) also reported weight loss at the time of presentation, and 57% had a concomitant psychiatric history. Diagnostic imaging most commonly used included duplex ultrasound (81%), computed tomography angiography (66%), angiography (57%), and magnetic resonance angiography (5%). Fourteen patients (67%) underwent multiple diagnostic studies. All patients underwent initial laparoscopic MAL release. Seven patients (33%) underwent subsequent celiac stent placement in the setting of recurrent or unresolved symptoms with persistent celiac stenosis at a mean interval of 49 days. Two patients required surgical bypass after an endovascular intervention failed. The 6-month freedom from symptoms was 75% and freedom from reintervention was 64%. Eighteen patients (81%) reported early symptom improvement and weight gain, and 66% were able to return to work.
Conclusions: A multidisciplinary treatment approach using initial laparoscopic release and subsequent stent placement and bypass surgery provides symptom improvement in most patients treated for MALS. The potential placebo effect, however, remains uncertain. A significant minority of patients will require reintervention, justifying longitudinal surveillance and prudent patient selection. Patients can anticipate functional recovery, weight gain, and return to work with treatment.
Copyright © 2015 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Gruber H, Loizides A, Peer S, Gruber I. Ultrasound of the median arcuate ligament syndrome: a new approach to diagnosis. Med Ultrason. 2012;14:5–9. - PubMed
-
- Mensink PB, van Petersen AS, Kolkman JJ, Otte JA, Huisman AB, Geelkerken RH. Gastric exercise tonometry: the key investigation in patients with suspected celiac artery compression syndrome. J Vasc Surg. 2006;44:277–81. - PubMed
-
- Jimenez JC, Harlander-Locke M, Dutson EP. Open and laparoscopic treatment of median arcuate ligament syndrome. J Vasc Surg. 2012;56:869–73. - PubMed
-
- Roseborough GS. Laparoscopic management of celiac artery compression syndrome. J Vasc Surg. 2009;50:124–33. - PubMed
-
- Vaziri K, Hungness ES, Pearson EG, Soper NJ. Laparoscopic treatment of celiac artery compression syndrome: case series and review of current treatment modalities. J Gastrointest Surg. 2009;13:293–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
