

Outcomes of nonresected main-duct intraductal papillary mucinous neoplasms of the pancreas
- PMID: 25759534
- PMCID: PMC4351216
- DOI: 10.3748/wjg.v21.i9.2658
Outcomes of nonresected main-duct intraductal papillary mucinous neoplasms of the pancreas
Abstract
Aim: To compare characteristics and outcomes of resected and nonresected main-duct and mixed intraductal papillary mucinous neoplasms of the pancreas (IPMN).
Methods: Over a 14-year period, 50 patients who did not undergo surgery for resectable main-duct or mixed IPMN, for reasons of precluding comorbidities, age and/or refusal, were compared with 74 patients who underwent resection to assess differences in rates of survival, recurrence/occurrence of malignancy, and prognostic factors. All study participants had dilatation of the main pancreatic duct by ≥ 5 mm, with or without dilatation of the branch ducts. Some of the nonsurgical patients showed evidence of mucus upon perendoscopic retrograde cholangiopancreatography or endoscopic ultrasound and/or after fine needle aspiration. For the surgical patients, pathologic analysis of resected specimens confirmed a diagnosis of IPMN with involvement of the main pancreatic duct or of both branch ducts as well as the main pancreatic duct. Clinical and biologic follow-ups were conducted for all patients at least annually, through hospitalization or consultation every six months during the first year of follow-up, together with abdominal imaging analysis (magnetic resonance cholangiopancreatography or computed tomography) and, if necessary, endoscopic ultrasound with or without fine needle aspiration.
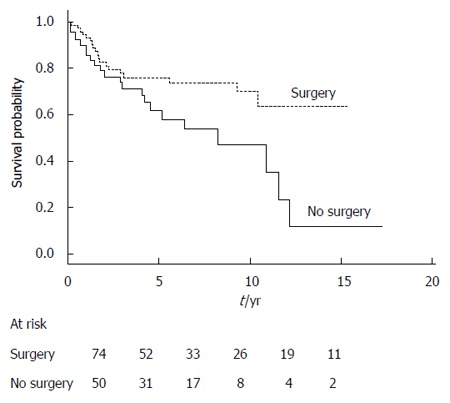
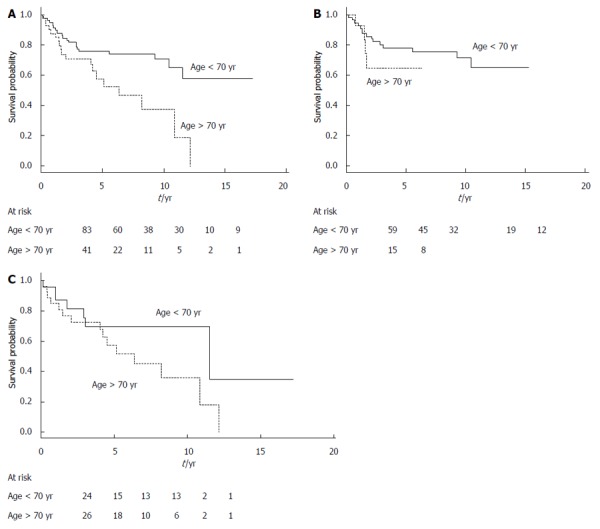
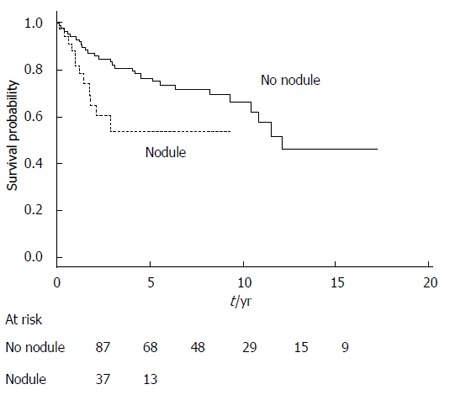
Results: The overall five-year survival rate of patients who underwent resection was significantly greater than that for the nonsurgical patients (74% vs 58%; P = 0.019). The parameters of age (< 70 years) and absence of a nodule were associated with better survival (P < 0.05); however, the parameters of main pancreatic duct diameter > 10 mm, branch duct diameter > 30 mm, or presence of extra pancreatic cancers did not significantly influence the prognosis. In the nonsurgical patients, pancreatic malignancy occurred in 36% of cases within a mean time of 33 mo (median: 29 mo; range: 8-141 mo). Comparison of the nonsurgical patients who experienced disease progression with those who did not progress showed no significant differences in age, sex, symptoms, subtype of IPMN, or follow-up period; only the size of the main pancreatic duct was significantly different between these two sub-groups, with the nonsurgical patients who experienced progression showing a greater diameter at the time of diagnosis (> 10 mm).
Conclusion: Patients unfit for surgery have a 36% greater risk of developing pancreatic malignancy of the main-duct or mixed IPMN within a median of 2.5 years.
Keywords: Main-duct intraductal papillary mucinous neoplasms; Natural history; Pancreatic surgery; Prognosis; Risk of malignancy.
Figures
References
-
- Hruban RH, Takaori K, Klimstra DS, Adsay NV, Albores-Saavedra J, Biankin AV, Biankin SA, Compton C, Fukushima N, Furukawa T, et al. An illustrated consensus on the classification of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol. 2004;28:977–987. - PubMed
-
- Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, Falconi M, Shimizu M, Yamaguchi K, Yamao K, Matsuno S. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006;6:17–32. - PubMed
-
- Tanaka M, Fernández-del Castillo C, Adsay V, Chari S, Falconi M, Jang JY, Kimura W, Levy P, Pitman MB, Schmidt CM, Shimizu M, Wolfgang CL, Yamaguchi K, Yamao K; International Association of Pancreatology. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology. 2012;12:183–197. - PubMed
-
- Schmidt CM, White PB, Waters JA, Yiannoutsos CT, Cummings OW, Baker M, Howard TJ, Zyromski NJ, Nakeeb A, DeWitt JM, et al. Intraductal papillary mucinous neoplasms: predictors of malignant and invasive pathology. Ann Surg. 2007;246:644–651; discussion 651-654. - PubMed
-
- Nagai K, Doi R, Kida A, Kami K, Kawaguchi Y, Ito T, Sakurai T, Uemoto S. Intraductal papillary mucinous neoplasms of the pancreas: clinicopathologic characteristics and long-term follow-up after resection. World J Surg. 2008;32:271–278; discussion 279-280. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
