

Neoadjuvant chemoradiotherapy followed by D2 gastrectomy in locally advanced gastric cancer
- PMID: 25759540
- PMCID: PMC4351222
- DOI: 10.3748/wjg.v21.i9.2711
Neoadjuvant chemoradiotherapy followed by D2 gastrectomy in locally advanced gastric cancer
Abstract
Aim: To investigate the efficacy of neoadjuvant chemoradiotherapy (NACRT) for resectability of locally advanced gastric cancer (LAGC).
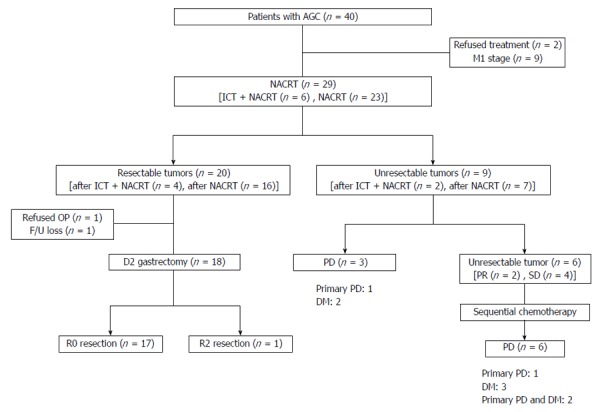
Methods: Between November 2007 and January 2014, 29 patients with LAGC (clinically T3 with distal esophagus invasion/T4 or bulky regional node metastasis) that were treated with NACRT followed by D2 gastrectomy were included in this study. Resectability was evaluated with radiologic and endoscopic exams before and after NACRT. Using three-dimensional conformal radiotherapy, patients received 45 Gy, with a daily dose of 1.8 Gy. The entire tumor extent and the regional metastatic lymph nodes were included in the gross tumor volume. Patients presenting with a resectable tumor after NACRT received a total or subtotal gastrectomy with D2 dissection. The pathologic tumor response was evaluated using Japanese Gastric Cancer Association histologic evaluation criteria. Postoperative morbidity was evaluated using the National Cancer Institute-Common Terminology Criteria for Adverse Events version 4.0. Overall survival (OS) and progression-free survival (PFS) rates were estimated using a Kaplan-Meier analysis and compared using the log-rank test.
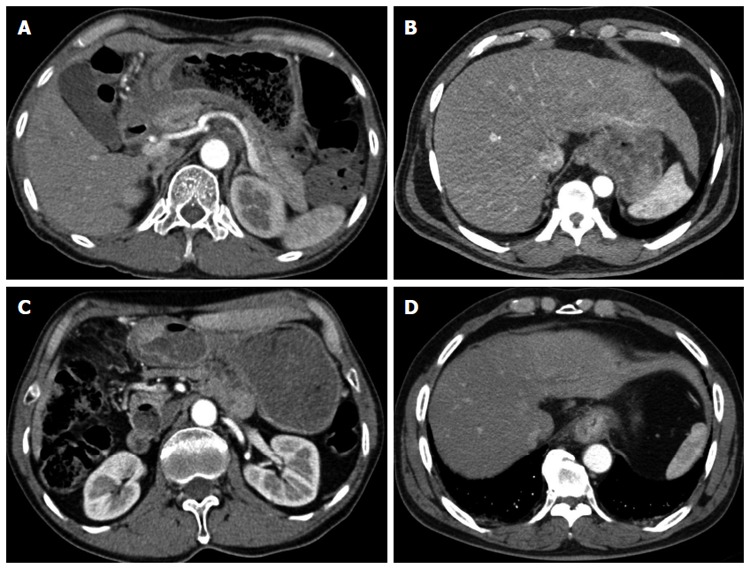
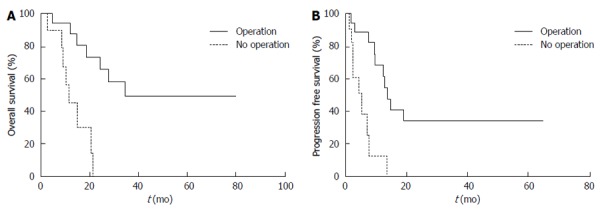
Results: All patients were assessed as unresectable cases. Twenty-four patients (24/29; 82.8%) showed LAGC on positron emission tomography-computed tomography (CT) and contrast-enhanced CT, whereas four patients (4/29; 13.8%) with vague invasion or abutment to an adjacent organ underwent diagnostic laparoscopy. One patient (1/29; 3.4%), initially assessed as a resectable case, underwent an "open and closure" after the tumor was found to be unresectable. Abutment to an adjacent organ (34.5%) was the most common reason for NACRT. The clinical response rate one month after NACRT was 44.8%. After NACRT, 69% (20/29) of patients had a resectable tumor. Of the 20 patients with a resectable tumor, 18 patients (62.1%) underwent a D2 gastrectomy. The R0 resection rate was 94.4% and two patients (2/18; 11.1%) showed a complete response. The median follow-up duration was 13.5 mo. The one-year OS and PFS rates were 72.4 and 48.9%, respectively. The one-year OS, PFS, local failure-free survival, and distant metastasis-free survival were higher in patients with a resectable tumor after NACRT (P < 0.001, P < 0.001, P < 0.001, and P = 0.078, respectively). No grade 3-4 late treatment-related toxicities or postoperative mortalities were observed.
Conclusion: NACRT with D2 gastrectomy showed a high rate of R0 resection and promising local control, which may increase the R0 resection opportunity resulting in survival benefit.
Keywords: Advanced gastric cancer; Combined modality therapy; D2 gastrectomy; Neoadjuvant chemoradiotherapy; Treatment outcome.
Figures
References
-
- Cheng CT, Tsai CY, Hsu JT, Vinayak R, Liu KH, Yeh CN, Yeh TS, Hwang TL, Jan YY. Aggressive surgical approach for patients with T4 gastric carcinoma: promise or myth? Ann Surg Oncol. 2011;18:1606–1614. - PubMed
-
- Cunningham D, Allum WH, Stenning SP, Thompson JN, Van de Velde CJ, Nicolson M, Scarffe JH, Lofts FJ, Falk SJ, Iveson TJ, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11–20. - PubMed
-
- Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med. 2001;345:725–730. - PubMed
-
- Yoshikawa T, Omura K, Kobayashi O, Nashimoto A, Takabayashi A, Yamada T, Yamaue H, Fujii M, Yamaguchi T, Nakajima T. A phase II study of preoperative chemotherapy with S-1 plus cisplatin followed by D2/D3 gastrectomy for clinically serosa-positive gastric cancer (JACCRO GC-01 study) Eur J Surg Oncol. 2010;36:546–551. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
