

IgG4-related autoimmune diseases: Polymorphous presentation complicates diagnosis and treatment
- PMID: 25759979
- PMCID: PMC4361802
- DOI: 10.3238/arztebl.2015.0128
IgG4-related autoimmune diseases: Polymorphous presentation complicates diagnosis and treatment
Abstract
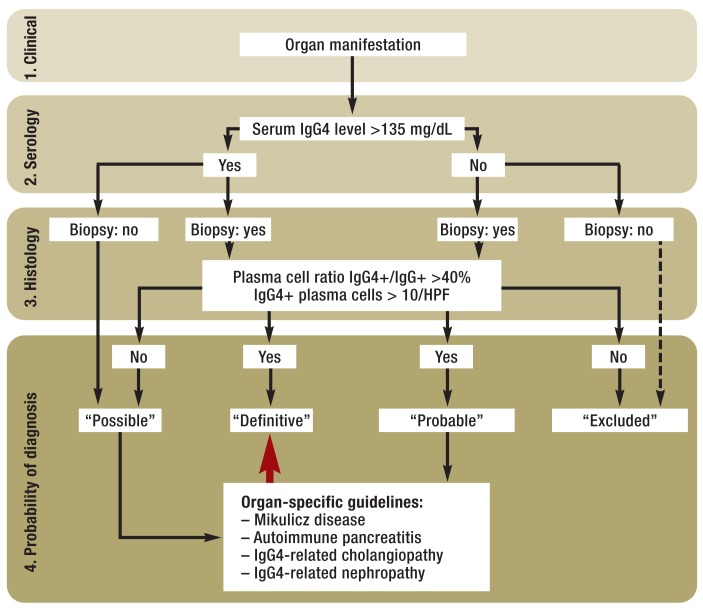
Background: IgG4-associated autoimmune diseases are systemic diseases affecting multiple organs of the body. Autoimmune pancreatitis, with a prevalence of 2.2 per 100,000 people, is one such disease. Because these multi-organ diseases present in highly variable ways, they were long thought just to affect individual organ systems. This only underscores the importance of familiarity with these diseases for routine clinical practice.
Methods: This review is based on pertinent articles retrieved by a selective search in PubMed, and on the published conclusions of international consensus conferences.
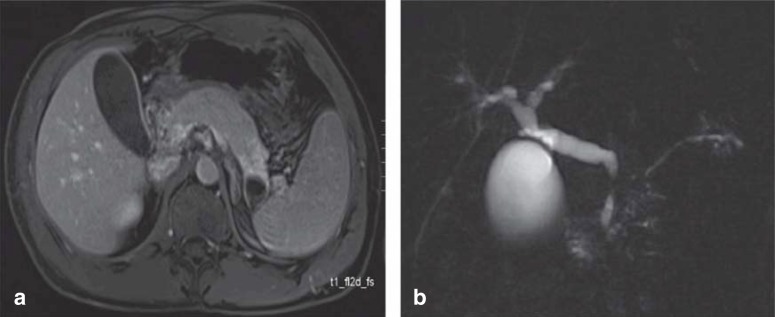
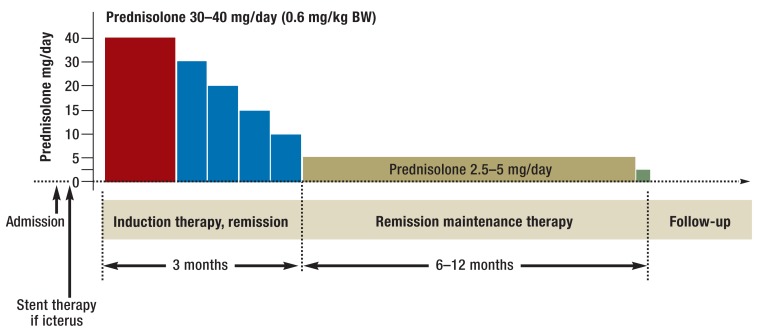
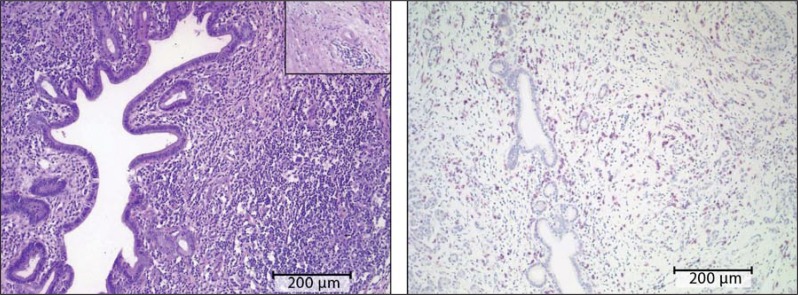
Results: The current scientific understanding of this group of diseases is based largely on case reports and small case series; there have not been any randomized controlled trials (RCTs) to date. Any organ system can be affected, including (for example) the biliary pathways, salivary glands, kidneys, lymph nodes, thyroid gland, and blood vessels. Macroscopically, these diseases cause diffuse organ swelling and the formation of pseudotumorous masses. Histopathologically, they are characterized by a lymphoplasmacytic infiltrate with IgG4-positive plasma cells, which leads via an autoimmune mechanism to the typical histologic findings--storiform fibrosis ("storiform" = whorled, like a straw mat) and obliterative, i.e., vessel-occluding, phlebitis. A mixed Th1 and Th2 immune response seems to play an important role in pathogenesis, while the role of IgG4 antibodies, which are not pathogenic in themselves, is still unclear. Glucocorticoid treatment leads to remission in 98% of cases and is usually continued for 12 months as maintenance therapy. Most patients undergo remission even if untreated. Steroid-resistant disease can be treated with immune modulators.
Conclusion: IgG4-associated autoimmune diseases are becoming more common, but adequate, systematically obtained data are now available only from certain Asian countries. Interdisciplinary collaboration is a prerequisite to proper diagnosis and treatment. Treatment algorithms and RCTs are needed to point the way to organ-specific treatment in the future.
Figures
Comment in
-
Unsuitable Terminology.Dtsch Arztebl Int. 2015 Jun 19;112(25):444. doi: 10.3238/arztebl.2015.0444a. Dtsch Arztebl Int. 2015. PMID: 26179018 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2015 Jun 19;112(25):444. doi: 10.3238/arztebl.2015.0444b. Dtsch Arztebl Int. 2015. PMID: 26179019 Free PMC article. No abstract available.
References
-
- Kamisawa T, Egawa N, Nakajima H. Autoimmune pancreatitis is a systemic autoimmune disease. Am J Gastroenterol. 2003;98:2811–2812. - PubMed
-
- Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012;25:1181–1192. - PubMed
-
- Uchida K, Masamune A, Shimosegawa T, Okazaki K. Prevalence of IgG4-related disease in Japan based on nationwide survey in 2009. Int J Rheumatol. 2012 www.hindawi.com/journals/ijr/2012/358371 (last accessed on 13. January 2015) - PMC - PubMed
-
- Fritz S, Bergmann F, Grenacher L, et al. Diagnosis and treatment of autoimmune pancreatitis types 1 and 2. Br J Surg. 2014;101:1257–1265. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical