

Treatment changes among older patients with dementia treated with antipsychotics
- PMID: 25759986
- PMCID: PMC6201312
- DOI: 10.1002/gps.4281
Treatment changes among older patients with dementia treated with antipsychotics
Abstract
Background: Prescribing practice patterns and factors associated with treatment changes in older patients initiating antipsychotic treatment for the behavioral and psychological symptoms of dementia is not well known.
Objectives: The objective of this study is to study 90-day prescribing practice patterns across the three most commonly prescribed antipsychotics.
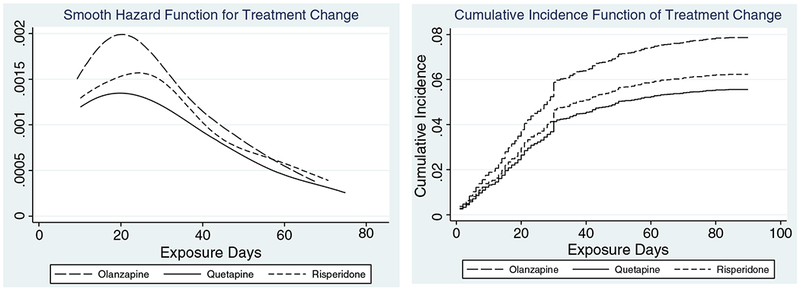
Methods: This is a retrospective study using national data from the US Department of Veterans Affairs (VA). The study included patients older than 65 years diagnosed with dementia who began outpatient treatment with an antipsychotic medication between 2005 and 2008. Patients were followed for 90 days from their antipsychotic start. The primary event of interest was changing to another psychotropic medication. Cumulative incidence of treatment change was determined with antipsychotic discontinuation and death as competing risks. Covariate-adjusted hazard ratios for treatment change were determined using competing risk regression models.
Results: During the study period, 15,435 patients initiated an atypical antipsychotic; 14,791 started olanzapine, quetiapine, or risperidone. Over half (55%) of the patients discontinued index treatment within 90 days, 36% continued, 3% died while on index treatment, and 6% changed to another psychotropic medication. Compared with quetiapine, the adjusted hazard of treatment change was higher by 43% (p = 0.005) for olanzapine and by 12% (p = 0.08) for risperidone.
Conclusion: The higher hazard of treatment change with olanzapine suggests patients either responded worse to or experienced more adverse events with olanzapine compared with quetiapine.
Keywords: atypical antipsychotics; dementia; older patients; treatment change.
Copyright © 2015 John Wiley & Sons, Ltd.
Conflict of interest statement
Conflict of interest
None declared.
Figures
References
-
- Ayalon L, Area’n PA, Alvidrez J 2005. Adherence to antidepressant medications in Black and Latino elderly patients. Am J Geriatr Psychiatry 13(7): 572–80. - PubMed
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. 1987. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40(5): 373–83. - PubMed
-
- Davis JM, Chen N, Glick ID. 2003. A meta-analysis of the efficacy of secondgeneration antipsychotics. Arch Gen Psychiatry 60(6): 553–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
