

Enhancing our understanding of current therapies for hepatitis C virus (HCV)
- PMID: 25761432
- PMCID: PMC4373591
- DOI: 10.1007/s11904-014-0243-7
Enhancing our understanding of current therapies for hepatitis C virus (HCV)
Abstract
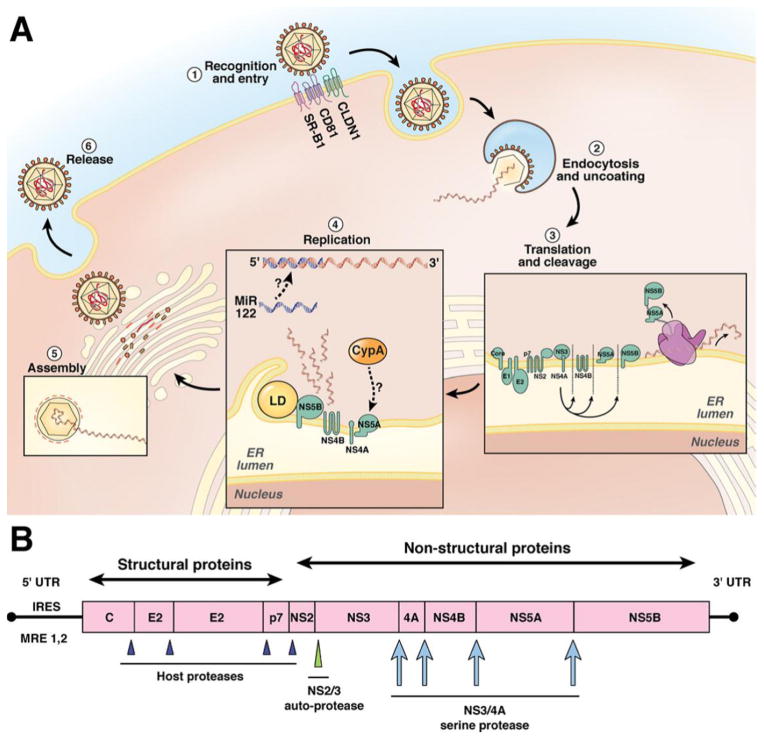
Great progress has been made in understanding the HCV genome and its molecular virology. This understanding has culminated in the development of direct-acting antiviral (DAA) agents targeting HCV viral proteins. Telaprevir (TVR) and boceprevir (BOC) were the first DAAs introduced for treatment of genotype 1 HCV in 2011; when used in combination with pegylated interferon (pegIFN) and ribavirin (RBV), these protease inhibitors improved efficacy in patients with chronic HCV infection compared to the traditional dual therapy. However, this combination was associated with adverse events that often led to early termination of therapy. In late 2013, the FDA approved a second wave of DAAs, sofosbuvir (SOF) and simeprevir (SMV). The use of SOF with SMV opened the door for IFN-free combination regimens. This combination was highly efficacious and well tolerated in patients with HCV genotype 1. Sofosbuvir and ledipasvir (LDV) fixed-dose oral combination (FDC) therapy, and paritaprevir/ritonavir, ombitasvir and dasabuvir ± RBV were recently approved, elevating sustained virologic response (SVR) rates to over 95 %. We are anticipating the approval of additional IFN-free regimens with comparable efficacy and tolerability but with the addition of pangenotypic coverage, fewer drug-drug interactions, and a high barrier to resistance. This review will summarize current management for chronic HCV infection.
Conflict of interest statement
Neliswa A. Gogela, Ming V. Lin, and Jessica L. Wisocky declare that they have no conflict of interest.
Figures
References
-
- Chevaliez S, Pawlotsky JM. HCV Genome and Life Cycle. In: Tan SL, editor. Hepatitis C Viruses: Genomes and Molecular Biology. Norfolk (UK): 2006.
-
- Choo QL, et al. Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science. 1989;244(4902):359–62. - PubMed
-
- Urbanus AT, et al. Trends in hepatitis C virus infections among MSM attending a sexually transmitted infection clinic; 1995–2010. AIDS. 2014;28(5):781–90. - PubMed
-
- Zielinski A. Sexual behaviour and the risk of HCV infection. Przegl Epidemiol. 2014;68(1):1–3. 99–100. - PubMed
-
- Smith BD, et al. Recommendations for the identification of chronic hepatitis C virus infection among persons born during 1945–1965. MMWR Recomm Rep. 2012;61(RR-4):1–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
